


Benign paroxysmal positional vertigo (BPPV) is a common diagnosis in our field. We know the drill: dislodged otoconia in the semicircular canals triggers brief but intense episodes of vertigo with head movements. But what if the classic picture doesn't quite fit? What if the Epley maneuver doesn't provide lasting relief?
It's time to expand our thinking beyond the crystals.
Vestibular Asymmetry: The Unsung Culprit
While BPPV is often attributed to otoconia, it's crucial to remember that any imbalance in vestibular function can lead to positional vertigo. This asymmetry can stem from various sources:
Vestibular neuritis/labyrinthitis: Inflammation affecting the inner ear or vestibular nerve.
Meniere's disease: Fluctuations in inner ear fluid dynamics.
Acoustic neuroma: A benign growth on the vestibular nerve.
Head injuries: Damage to the inner ear or vestibular pathways.
Age-related decline: Gradual deterioration of vestibular function.
When one vestibular system is weaker (hypofunction), it disrupts the delicate balance of signals sent to the brain about head position. This can trigger vertigo, especially when challenged by specific head movements. Remember, the semicircular canals are interconnected, so dysfunction in one can affect its paired canal on the opposite side, further contributing to the imbalance.
Vertebral Artery: An Overlooked Connection?
Recent discussions have highlighted the potential role of vertebral artery issues in contributing to vertigo, including positional vertigo. Here's why this is relevant:
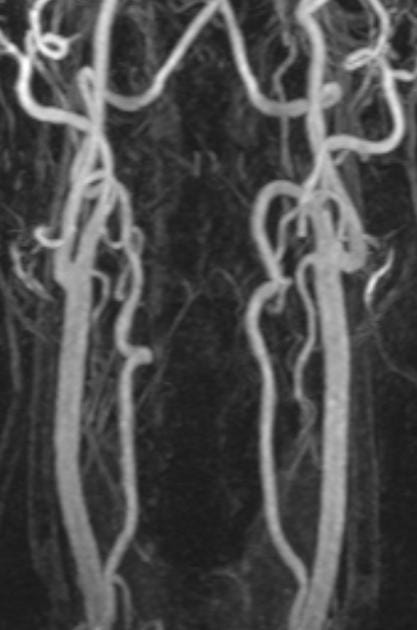
Vertebral Artery Tortuosity: Twisting or kinking of the vertebral artery, common in older adults, can reduce blood flow to the brainstem and cerebellum—areas vital for balance and spatial orientation. While not directly supplying the vestibular system, this reduced blood flow (vertebrobasilar insufficiency or VBI) can affect vestibular nuclei function, potentially leading to dizziness and vertigo.
Mechanical Compression: Head rotation can compress the vertebral arteries, particularly at the atlantoaxial (C1-C2) or subaxial levels. This can trigger transient VBI, with symptoms ranging from dizziness to vertigo and even stroke in severe cases. Could this mechanically induced vertigo be mistaken for BPPV, mainly if triggered by specific head positions?
Implications for Vestibular Professionals
Thorough Assessment: Don't jump to conclusions! A comprehensive vestibular evaluation is essential for pinpointing positional vertigo's root cause. Consider caloric testing, VEMPs, and imaging (MRI/CT angiography) to assess peripheral and central vestibular function and vertebral artery anatomy.
Individualized Treatment: If the underlying cause is vestibular asymmetry or VBI, maneuvers like the Epley might not be effective. Focus on addressing the root problem: vestibular rehabilitation, medication for Meniere's disease, or managing vascular risk factors for VBI.
Patient Education: Explain to patients that their positional vertigo may not be solely due to crystals. This helps manage expectations and encourages adherence to a tailored treatment plan.
Expanding Our Understanding
We can refine our diagnostic and treatment approaches by recognizing that positional vertigo can arise from various causes beyond dislodged otoconia. Let's embrace a more holistic perspective, considering the intricate interplay between the vestibular system, vascular health, and neck biomechanics. This will ultimately lead to better outcomes for our patients.
What are your thoughts? We encourage you to share your experiences and insights in the comments below! Your contributions can help us all learn and grow in our understanding of vestibular disorders.