


Beyond the Beat: Unpacking Geotropic and Apogeotropic Nystagmus in BPPV

As vestibular professionals, we routinely assess patients experiencing Benign Paroxysmal Positional Vertigo (BPPV). When observing nystagmus during these assessments, terminology can quickly become complex, as it intertwines descriptions of horizontal, vertical, and torsional components with terms like 'up-beating,’ 'down-beating,‘ 'right-beating,‘ 'left-beating,' and then the ever-present 'geotropic' and 'apogeotropic.’ This often leads to confusion.
Our goal here is to demystify these gravitational terms and emphasize a fundamental principle:
'All BPPV-induced nystagmus demonstrates either geotropic or apogeotropic characteristics, depending on the patient's perspective and position during testing.'
Historically, Dix and Hallpike, when describing their provocative maneuver in 1952, indeed characterized the positional nystagmus they observed. The specific terms 'geotropic' and 'apogeotropic' became standardized in vestibular science to precisely describe the fast phase of nystagmus relative to the Earth's gravitational pull, offering a crucial layer of diagnostic understanding beyond simply the beating direction in the visual field.
Understanding the Core Terminology:
Let's establish the definitions clearly:
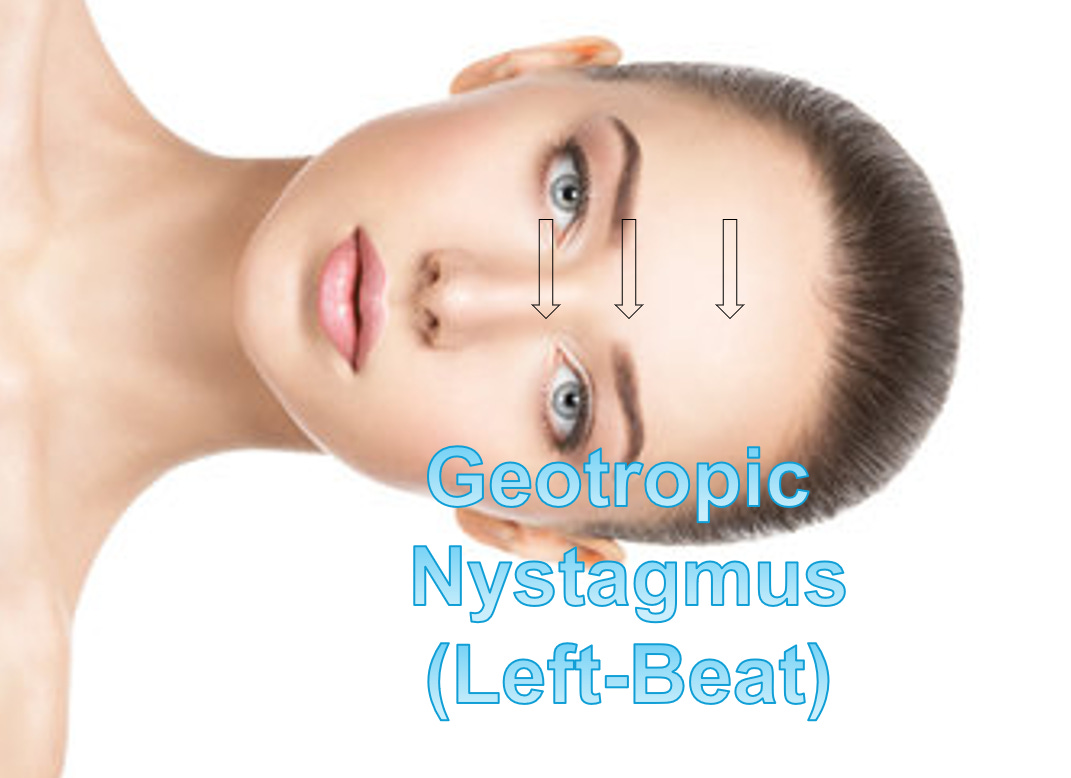
Geotropic: This term describes nystagmus, where the fast phase beats towards the Earth's center of gravity.
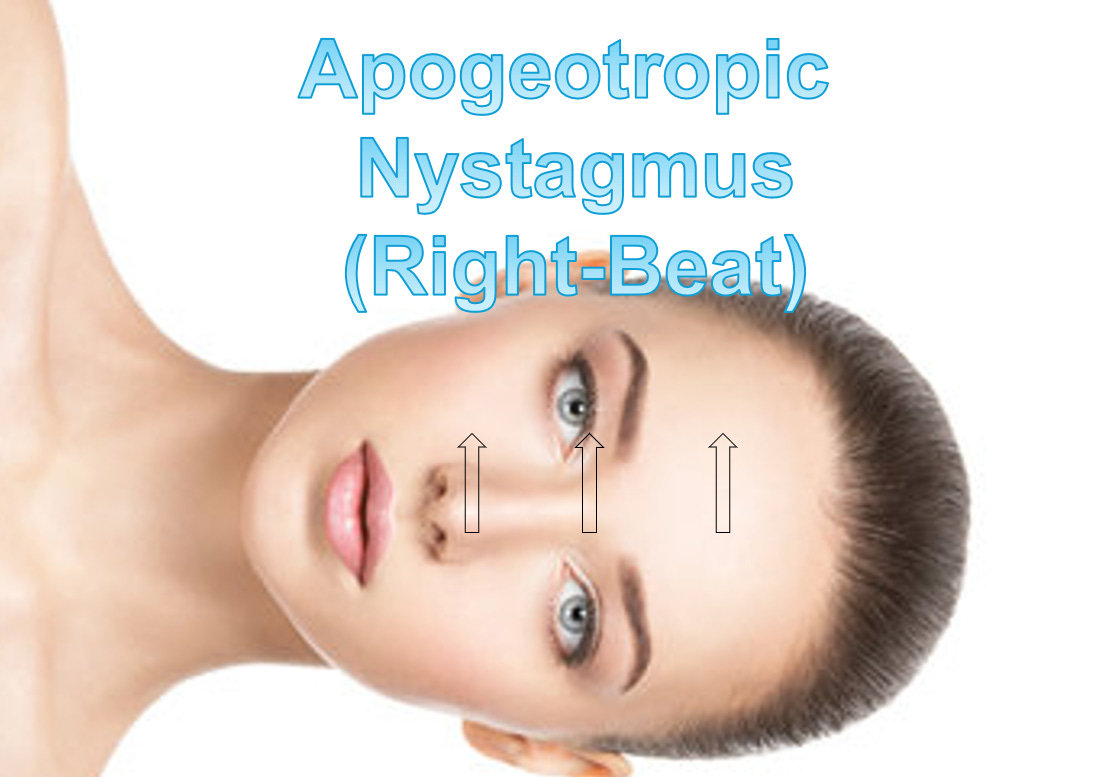
Apogeotropic: This term describes nystagmus, where the fast phase beats away from the Earth.

NOTE: We must address the term 'ageotropic'. While occasionally used, we do not prefer it in precise clinical descriptions of nystagmus. 'A-' typically means 'without' (as in Latin), implying a lack of motion, which fundamentally contradicts the presence of nystagmus. Therefore, we focus on the directional descriptors: geotropic or apogeotropic.
Applying the Concepts: Vertical Canals in the Dix-Hallpike Position
When assessing for vertical canal BPPV, we ALWAYS USE the Dix-Hallpike position. Here's how nystagmus aligns with geotropic/apogeotropic:
Posterior Canal BPPV: For classic posterior canal BPPV, placing the patient into the Dix-Hallpike position (e.g., 'right Dix-Hallpike' for a right posterior canal) typically elicits an 'up-beating' and 'torsional' nystagmus (e.g., 'up-beat right-torsion'). Because the head is back and the nystagmus beats 'towards the eyebrows' (i.e., 'towards the Earth's surface' relative to the patient's orientation), this describes geotropic nystagmus. The same applies to a left posterior canal, causing 'upbeat left-torsion' in a left Dix-Hallpike maneuver.

Anterior Canal BPPV: If we observe nystagmus from an anterior canal BPPV in the Dix-Hallpike position, it presents as 'down-beating' and 'torsional' (e.g., 'down-beat right-torsion' in a right Dix-Hallpike). Since this nystagmus beats 'towards the chin' (i.e., 'away from the Earth's surface' relative to the patient's orientation), this describes apogeotropic nystagmus.

Applying the Concepts: Horizontal Canals in the Supine Head Roll or Sidelying Position
The same principles apply to horizontal canal BPPV, which we assess by conducting either the Supine Head Roll Test or the Sidelying Test. In the Supine Head Roll Test, the patient lies supine, and their head turns to either side. In the Sidelying Test, the patient lies directly on their side.
When a patient lies on their Right Side:
If the nystagmus is 'right-beating horizontal' (beating 'towards the Earth/ground'), it is geotropic nystagmus.

If the nystagmus is 'left-beating horizontal' (beating 'away from the Earth/ceiling'), it is apogeotropic nystagmus.


When a patient lies on their Left Side:
If the nystagmus is 'left-beating horizontal' (beating 'towards the Earth/ground'), it is geotropic nystagmus.
If the nystagmus is 'right-beating horizontal' (beating 'away from the Earth/ceiling'), it is apogeotropic nystagmus.


Beyond the Usual: Unique Presentations
This framework also helps us understand less common but critical presentations. For example, some patients present with what we term a 'non-ampullary posterior canal BPPV,’ where the debris is moving ampullopetally in the PSC, often leading to what some refer to as 'Apogeotropic Posterior Canal BPPV. ’ Understanding the location and direction of movement of the debris (AMPULLOPETAL vs. AMPULLOFUGAL) allows for precise differentiation.
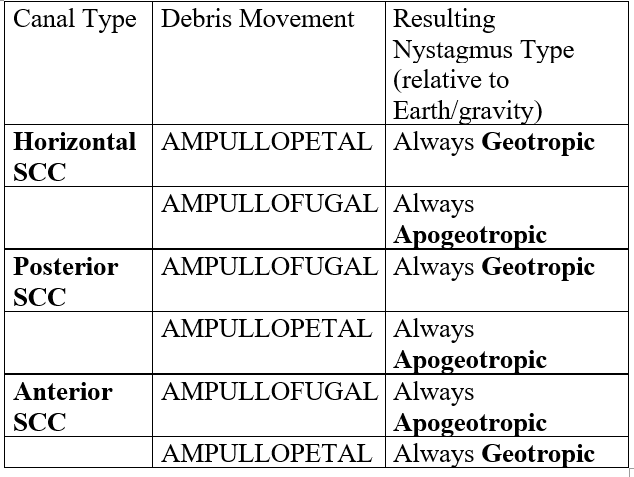
The Nystagmus Map: Debris Movement and Gravitational Direction
The direction of debris movement within any semicircular canal (AMPULLOPETAL or AMPULLOFUGAL) directly dictates whether the resulting nystagmus will be geotropic or apogeotropic in specific test positions. The table below summarizes these key relationships - stop and review the table if listening:
Conclusion:
By distinguishing between the horizontal, vertical, and torsional components of nystagmus and the gravitational direction (geotropic versus apogeotropic), vestibular professionals can achieve a more precise diagnosis and develop more effective treatment strategies. This deeper understanding moves beyond simple pattern recognition, allowing us to accurately interpret complex eye movements and tailor our interventions to the specific pathophysiology of BPPV. Mastering this terminology is fundamental to advancing our shared mission in vestibular rehabilitation.
Thank you for this review. When you have a complex case like I did several weeks ago - one has to go back to the basics and think through each test and what they are seeing. Guidance from a veteran vestibular PT helped walk me through the case and we were able to help the patient immensely.
** take away** know the basics and help fellow therapists when we can 🙌💛🙌
Do you have any info on severe balance and spacial awareness issues for prople that have bi-lateral cochlear implants? No dizziness or vertigo.