

Beyond the Neck: Why the ‘Hoffmann and Trömner’ Signs Belong in Every PT’s Bedside Screen


Imagine a scenario where a patient with a subtle but serious nervous system issue visits a physical therapist and receives standard care. Unfortunately, a key UMN lesion is overlooked, leading to delayed treatment and prolonged recovery. Such situations underscore the urgent need for comprehensive bedside screening to expedite differential diagnosis and improve patient outcomes. In physical therapy practice, clinicians frequently operate at the intersection of multiple specialties. Whether treating patients in acute care, neurological rehabilitation, or post-concussion settings, it is essential that bedside screening effectively detects central nervous system dysfunction. Two of the most reliable, yet frequently overlooked, tests for upper motor neuron (UMN) involvement are the ‘Hoffmann sign’ and the ‘Trömner sign’. (Reliability and Repeatability of the Hoffmann Sign, 2012, pp. 118-121)
The Two Sides of the Same Coin
Both tests are designed to elicit a specific pathological reflex: involuntary flexion of the thumb and index finger, resembling a pincer-like twitch. This response indicates hyperreflexia and suggests irritability within the spinal cord or brain. (Whitney, 2025)
1. The ‘Hoffmann Sign’ (The Downward Flick)
This test focuses on stimulating the finger flexors.
Technique: Stabilize the patient’s middle finger at the distal interphalangeal (DIP) joint. Use your thumbnail to sharply flick the patient’s middle fingernail downward with a flick distance of approximately 1 cm. Ensure the finger is held at a slight angle to avoid excessive force and maintain consistency.
Mechanism: This creates a sudden stretch of the finger flexors.
2. The ‘Trömner Sign’ (The Upward Tap)
This test is performed in reverse to the Hoffmann test. Rather than flicking downward, the examiner taps upward.
Technique: Hold the patient’s middle finger in a relaxed, partially extended position. With your other hand, sharply tap or flick the volar surface (the pad) of the middle fingertip upward toward extension.
Mechanism: This provides a quick stretch to the finger flexors by tapping from the palmar side.
Interpreting the Results at the Bedside
Regardless of which test is selected, the clinical significance is consistent:
‘Positive Sign’: Observation of the thumb and index finger flexing or adjoining in a rapid twitch indicates upper motor neuron irritability. This is supported by sensitivity and specificity ranges in clinical assessments, such as cervical myelopathy, which show sensitivity of approximately 60–80% in detecting conditions^1. Such evidence-based interpretation underscores the importance of valuing a positive sign in clinical practice.
‘Negative Sign’: The thumb and index finger remain motionless despite the stimulus to the middle finger, suggesting a normal and intact reflex arc.
Why This Matters for Post-Concussion and Stroke
In patients with recent concussion or suspected stroke, these tests offer immediate clinical insight. A positive Trömner or Hoffmann sign, particularly if unilateral, represents a significant upper motor neuron red flag that is frequently overlooked during standard strength screening. (Chang et al., 2011)
The Grading Criteria
To accurately grade these tests, you must observe the symmetry and the intensity of the response:
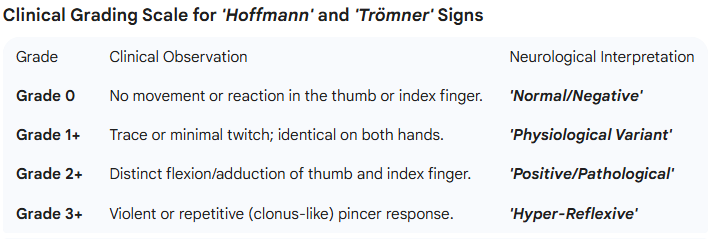
Grade 0 (Absent): No movement occurs in the thumb or index finger. This is the expected normal finding.
Grade 1+ (Symmetric/Physiological): A very slight twitch occurs, but it is identical on both the left and right hands. In patients with generalized hyperreflexia (without pathology), this may be a normal variant.
Grade 2+ (Positive/Pathological): A distinct, involuntary flexion or adduction of the thumb and index finger occurs.
Grade 3+ (Hyper-Reflexive/Clonus): The pincer movement is violent or repetitive (clonus-like) upon a single stimulation.
Clinical Grading Table
Key Clinical Takeaway
Always prioritize symmetry in your grading. A Grade 2+ result that appears only on the right side is far more clinically significant than a Grade 1+ result found on both sides. In the context of post-concussion or stroke, any asymmetric Grade 2+ or higher is a red flag that warrants an immediate referral.
By using this structured grading system, you provide clear, objective data to the rest of the medical team, ensuring the patient’s neurological status is tracked with precision.
Professional Documentation: The SOAP Note
When these signs are identified, accurate documentation is essential to facilitate appropriate medical follow-up. The following examples can guide clinical reporting:
Objective (O)
Special Tests: Hoffmann +R/−L; Trömner +R/−L.
‘Neurological Screen: Brisk DTRs (3+) noted at the (R) brachioradialis; positive Hoffmann’s sign noted unilaterally on the (R) side.’
Assessment (A)
‘Patient presents with signs of upper motor neuron involvement as evidenced by a positive (R) Hoffmann’s and Trömner’s sign. These findings, in conjunction with reported hand clumsiness and gait ataxia, suggest central nervous system irritability and require medical correlation.’
Plan (P)
Continue with the current plan of care for post-concussion symptoms. Educate the patient on the significance of unilateral positive Hoffmann and Trömner signs, including the potential need for further neurological imaging, to support informed, shared decision-making in their care. Will contact the referring physician today to discuss the findings for additional evaluation.
Clinical Demonstration
Observe both hand positions and pincer responses in this short clinical video:
Hoffman’s Test and Trömner’s Sign for UMN Lesions
Mastery of both the upward tap of the Trömner sign and the downward flick of the Hoffmann sign ensures that bedside screening remains thorough, professional, and precise. To incorporate these tests into your routine, challenge yourself to try both signs on your following clinic list and note any surprises. This practical approach can help turn theory into habit, enhancing your diagnostic skills with every patient.
References
2012). Reliability and Repeatability of the Hoffmann Sign. Journal of Clinical Neuroscience 19(1), pp. 118-121. https://doi.org/10.1016/j.jocn.2011.06.019
Whitney, E. (2025). Hoffmann’s Sign. StatPearls Publishing. https://pubmed.ncbi.nlm.nih.gov/31424740/
Chang, C., Chang, K. & Lin, S. (2011). Quantification of the Trömner signs: a sensitive marker for cervical spondylotic myelopathy. European Spine Journal 20(6). https://doi.org/10.1007/s00586-010-1681-6