


Benign paroxysmal positional vertigo (BPPV) is a common cause of peripheral vertigo, often triggered by specific head movements. While BPPV typically presents with characteristic features, it can occasionally mimic central positional vertigo, posing diagnostic challenges. This article highlights the nuances of distinguishing between these two conditions, thereby enabling physical therapists to make accurate diagnoses and provide optimal patient care.
The BPPV Conundrum: When it Masquerades as Central
BPPV, arising from displaced otoconia (calcium carbonate crystals) within the inner ear, usually manifests with brief, intense episodes of vertigo and nystagmus triggered by specific head positions. However, atypical presentations can blur the lines between BPPV and central positional vertigo.
Atypical nystagmus: Although BPPV typically exhibits torsional-rotatory nystagmus, variations like horizontal or vertical nystagmus can occur, resembling patterns seen in central vertigo.
Prolonged symptoms: While BPPV episodes are usually short-lived, lasting less than a minute, they can occasionally persist for longer durations, raising suspicion for a central cause.
Non-specific symptoms: BPPV can sometimes present with non-specific symptoms like nausea, imbalance, and disorientation, which can overlap with those seen in central vertigo.
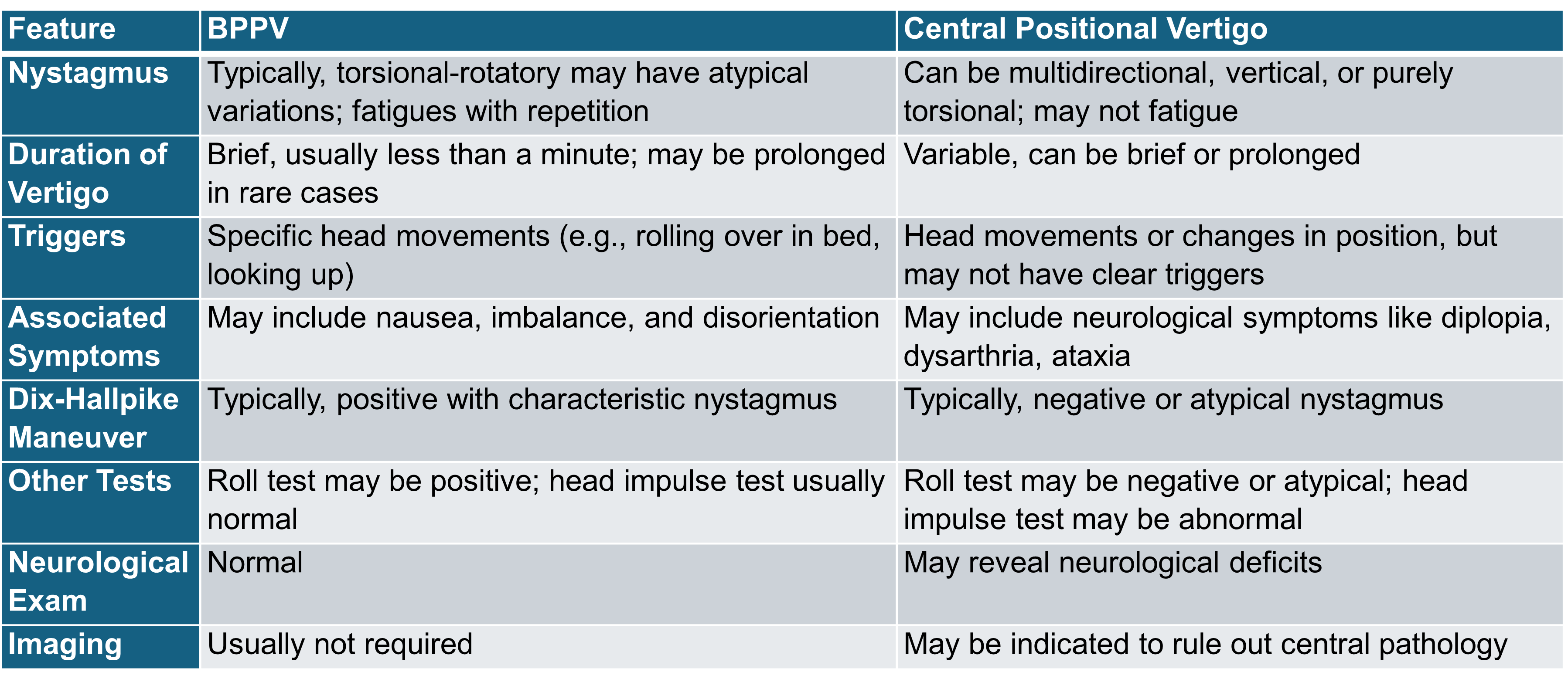
Distinguishing BPPV from Central Vertigo: Key Differentiators
Despite these potential overlaps, careful clinical assessment and specific tests can help unveil the true nature of the positional vertigo.
The Physical Therapist's Role: Navigating the Diagnostic Maze
As a physical therapist specializing in dizziness, your expertise in recognizing these subtle distinctions is invaluable. A thorough history, meticulous observation of nystagmus during positional testing, and a comprehensive neurological examination are crucial for accurate diagnosis.
When BPPV is suspected, the Dix-Hallpike maneuver is a powerful diagnostic tool. A positive test with characteristic nystagmus strongly suggests BPPV, thereby facilitating effective treatment with canalith repositioning maneuvers.
If central positional vertigo is suspected, prompt referral for further neurological evaluation is warranted. Imaging studies, such as MRI or CT scans, may be necessary to identify underlying brain or brainstem pathology.
Empowering Patients: Knowledge is Key
Beyond diagnosis and treatment, educating patients about their condition empowers them to participate actively in their recovery. Explain the differences between BPPV and central vertigo, emphasizing the benign nature of BPPV and the importance of adhering to any recommended treatment plans.
By combining your clinical expertise with effective patient education, you can guide individuals with positional vertigo toward improved balance, reduced symptoms, and enhanced quality of life. Remember, accurate diagnosis is the cornerstone of successful management, and your vigilance in differentiating BPPV from central positional vertigo is vital for ensuring optimal patient outcomes.
References
Central Positional Vertigo
Lin, J. C., Lin, Y. S., Huang, C. C., Lin, H. C., & Wang, S. J. (2023). Acute positional vertigo in the emergency department—peripheral vs. central positional nystagmus. Frontiers in Neurology, 14. https://doi.org/10.3389/fneur.2023.1266778
Central positional vertigo (P6.045). (2018). American Academy of Neurology Annual Meeting.
BPPV
Balaban, C. G., Kerber, K. A., & Schubert, M. C. (2024). Residual dizziness after BPPV management: Exploring pathophysiology and treatment beyond canalith repositioning maneuvers. Frontiers in Neurology, 15.
Wang, H., Liu, S., Zhang, H., Zhao, Z., & Zhang, J. (2023). Global research trends in benign paroxysmal positional vertigo: A bibliometric analysis. Frontiers in Neurology, 14.
Mazza, T., Mandalà, M., Lacquaniti, F., & Valli, P. (2023). Treatment of posterior benign paroxysmal positional vertigo is efficient and safe with a new mechanical rotational chair. Frontiers in Neurology, 14.