
Clinical Analysis: The Intersection of Polypharmacy and the Sensory Pivot in Geriatric Vestibular Care


Treating a 110-pound, 81-year-old female presenting with 8/10 nausea intensity requires a sophisticated understanding of pharmacological contraindications, especially regarding the inhibition of metabolic pathways and the cumulative effect of anticholinergic medications. When a patient presents with a lifelong history of motion sickness that remains despite GI intervention (‘Pantoprazole’) and has already failed standard antiemetics like ‘Ondansetron’, the clinical focus must shift toward the hierarchy of the central nervous system.
Comprehensive Pharmacological Constraints
The introduction of vestibular suppressants in this specific case poses a high risk to the patient’s systemic integrity. We must examine the following drug-to-drug interactions:
Paroxetine (SSRI) Interaction: ‘Paroxetine’ is a potent CYP2D6 inhibitor. This enzyme is responsible for processing many antihistamines and vestibular suppressants. Adding ‘Meclizine’ or ‘Cyclizine’ to her current ‘Paroxetine’ regimen will likely lead to metabolic inhibition, causing the suppressant’s serum levels to spike. In a low-weight geriatric patient, this significantly increases the risk of extreme lethargy and respiratory depression.
Failure of Ondansetron (Zofran): The lack of therapeutic benefit from ‘Ondansetron’ suggests that the nausea is not mediated through the typical peripheral or chemoreceptor trigger zone pathways. However, any further use of serotonergic agents must be monitored closely to avoid Serotonin Syndrome, given her current ‘Paroxetine’ dosage.
Antihistamine Accumulation: The patient is already taking a daily non-drowsy antihistamine. Adding ‘Meclizine’ or ‘Cyclizine’ creates a cumulative anticholinergic load. This frequently manifests as ‘brain fog’, urinary retention, and a dangerously high fall risk.
The Scopolamine Contraindication: ‘Scopolamine’ patches remain strictly discouraged in the geriatric population due to the high incidence of acute delirium, hallucinations, and urinary retention.
Pantoprazole and GI Considerations: While the patient is on Pantoprazole for a history of repaired ulcers, the 8/10 nausea intensity warrants a careful differential diagnosis to ensure the symptoms are vestibular rather than a primary GI flare-up.
The Sensory Pivot: A Reorganization of the Hierarchy
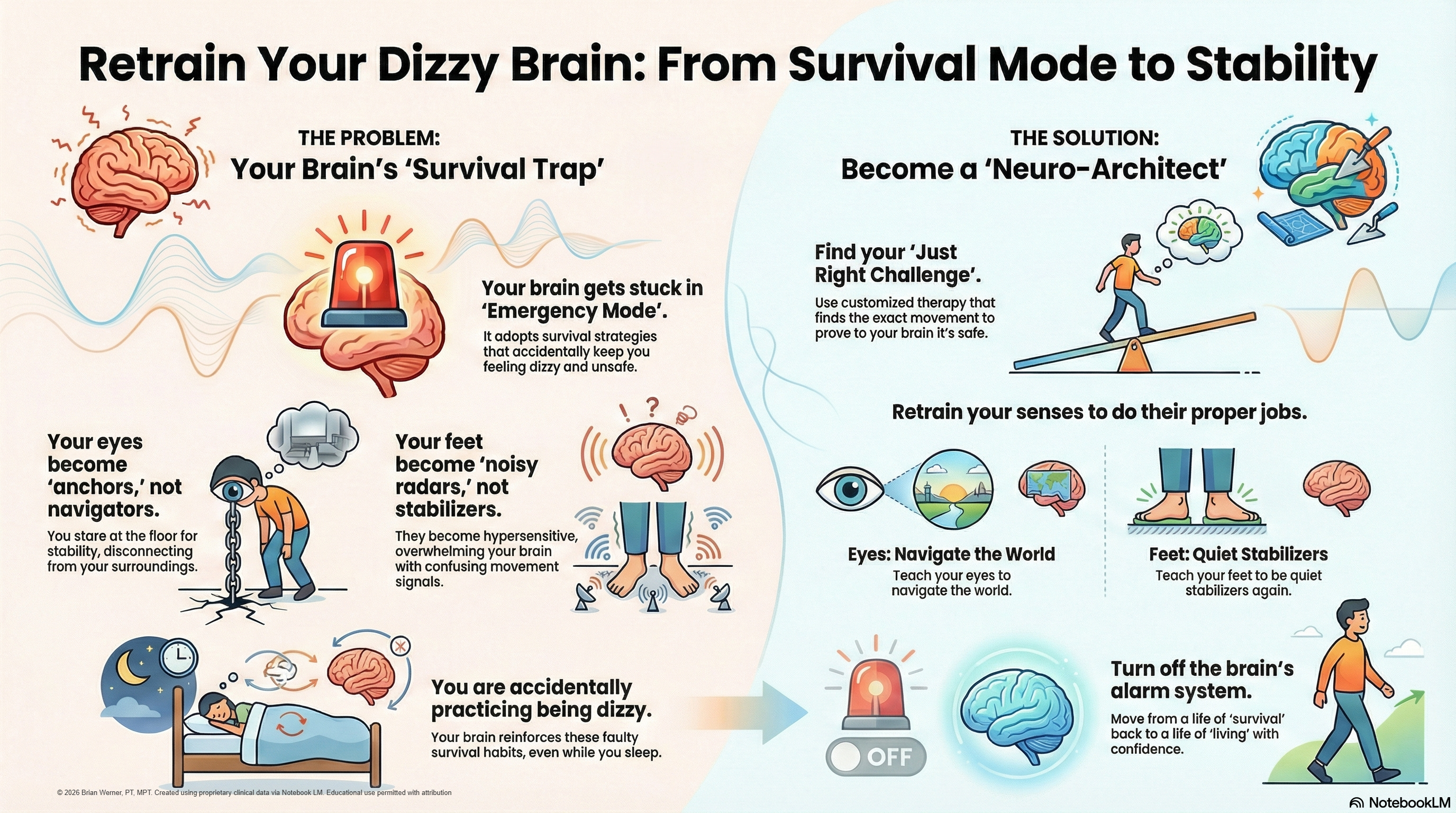
When a patient becomes movement-intolerant, the brain endures a major reorganization known as the sensory pivot. As the patient limits activity to avoid nausea, the brain begins to downregulate vestibular input. This creates a gap that the brain fills through a maladaptive sensory strategy.

Visual Dependency: From Navigation to Stabilization
The brain compensates by upregulating the visual system. However, instead of using vision for its primary role—navigation—it transitions the visual system into a stabilizer. The patient begins to use their eyes to ‘anchor’ themselves to their surroundings. This state of visual dependency means that any movement in the visual field is interpreted as a threat to postural integrity, triggering severe nausea through a constant sensory discrepancy.
Somatosensory Shift: The Radar Effect
Simultaneously, the somatosensory system experiences a transformation from a silent stabilizer to a high-gain navigator—a ‘radar’ system. The patient develops a strong surface dependency, in which the brain overinterprets every minor change in tactile input. This hyper-vigilance keeps the nervous system in a state of constant alarm.
Clinical Management and Strategy
To facilitate a return to function, the clinician must move away from suppressive pharmacological models and focus on the nervous system’s microenvironment. Because the present medication regimen—including ‘Paroxetine’, ‘Pantoprazole’, and a daily antihistamine—limits our pharmacological options, we must focus on the sensory process. Our strategy remains to:
Facilitate a more accurate integration of sensory input via addressing the mismatch between what the eyes see and what the body feels.
Support the transition of the visual system back to its primary navigating role, reducing the patient’s reliance on vision as a stabilizer.
Optimize signaling integrity between the vestibular nuclei and the cortex to encourage the brain to trust internal balance cues once again.
Coordinate the downregulation of somatosensory gain, returning it from a high-alert navigator to its natural role as a silent stabilizer.
Protect the balance system’s integrity by avoiding high-risk medications that impair the brain’s ability to recalibrate.
By dealing with the underlying sensory pivot rather than just masking the 8/10 nausea with sedative drugs, we provide a safer, more sustainable path to stability for the geriatric patient.