
Decoding BPPV: When Nystagmus Defies the Textbook (and the Dynamic Nature of Debris)


Introduction:
Hello, fellow vestibular explorers! As a physical therapist deeply immersed in the world of balance disorders, I'm constantly reminded that the inner ear is a master of surprises. The unexpected twists and turns in our exploration of vestibular disorders keep us engaged and intrigued. Recently, a student's insightful question led to a fascinating dive into the nuances of BPPV and nystagmus.
Picture this: A patient with suspected BPPV, showing negative Dix-Hallpike tests on both sides, yet reporting increased dizziness upon sitting, without visible nystagmus. The supine head roll test yielded no adverse result on the left but a positive one on the right, revealing rotational nystagmus—a twist in the tale.
The student's query: 'Why rotational nystagmus during a supine head roll test?'
Setting the Stage: Dizziness and the Vestibular Landscape
First, I emphasized the vital importance of defining 'dizziness.' It's a broad term encompassing vertigo, imbalance, lightheadedness, motion sickness, and even behavioral responses. In the context of BPPV, we must also remember that it often arises from degenerative changes in the inner ear, meaning symptoms can be multifaceted. Also, patient anxiety can heavily influence symptom reporting.
It is also important to remember that habituation to testing maneuvers can occur.
The Core Question: Unpacking Rotational Nystagmus
Here's where the anatomical puzzle pieces come into play. The rotational nystagmus observed during the supine head roll test can be attributed to these key factors:
The Interconnected Canals: It's crucial to understand that the supine head roll test, while primarily targeting the horizontal canals, doesn't operate in complete isolation.
The inner ear's intricate structure means that debris within the vertical canals can also be stimulated during this test.
Just as the Dix-Hallpike can excite the horizontal canals, the supine head roll can influence the vertical.
To help visualize this, search online for images of the inner ear, paying close attention to the spatial relationship of the semicircular canals. Viewing an inner ear diagram will significantly help us understand this concept.
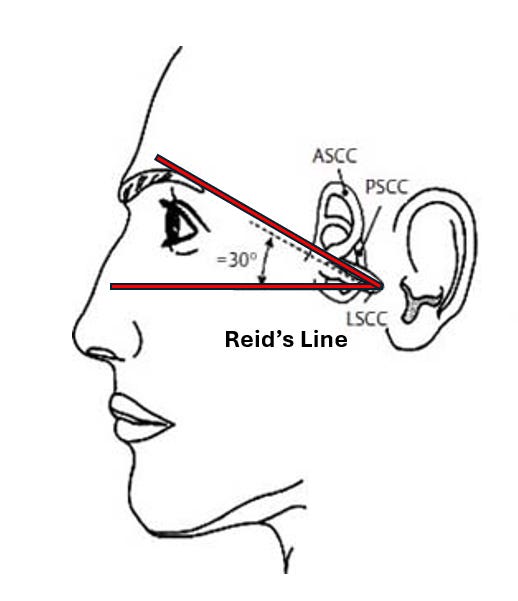
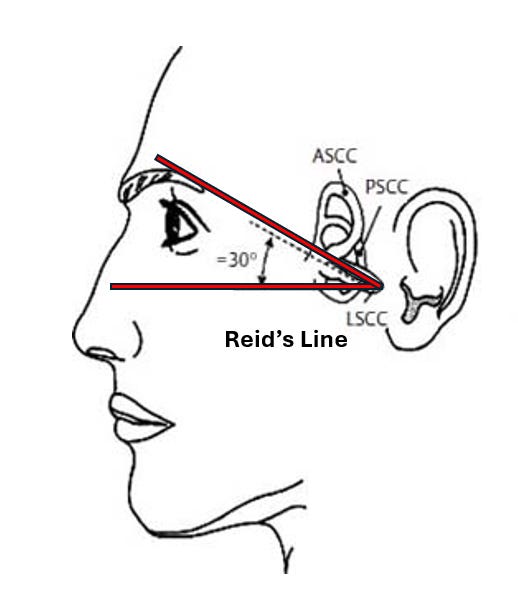
Reid's Line and Torsional Nuances: The horizontal canal isn't perfectly horizontal. It's angled approximately 30 degrees off the transverse plane, a concept known as Reed's line.
This angulation can introduce a torsional component to the nystagmus, potentially accompanied by a strong horizontal right/left beat.
The canal's orientation can cause a rotational element in the eye movements.
Expanding on the Nuances: Debris Location and Variable Responses
One of the most crucial aspects of understanding BPPV is recognizing the dynamic nature of canalithiasis. The debris within the semicircular canals doesn't remain static; it shifts and settles in various locations. This variability can lead to seemingly paradoxical test results, where a patient might exhibit nystagmus during a supine head roll test but not during a Dix-Hallpike or vice versa. Understanding this dynamic nature empowers us to interpret test results accurately and tailor treatment effectively.
Think about this: A piece of debris might be positioned deep within the posterior canal, too far down to elicit a response during the Dix-Hallpike maneuver. However, when the patient is placed in the supine head roll position, the canal's unique angulation and the altered gravitational forces can shift that same piece of debris, triggering a nystagmus response.
Conversely, debris located in a specific area of the horizontal canal may only be mobilized by the supine head roll while remaining undisturbed during the Dix-Hallpike.
Discarding that debris that always occupies a single, predictable location is vital. Debris fields can exist in multiple areas within the canals, each capable of producing distinct responses depending on the test position. This understanding is paramount for interpreting test results accurately and tailoring treatment effectively.
This means that a negative test does not always mean there is no BPPV. It just means that the debris was not in a place to be stimulated by the test maneuver.
By acknowledging the potential for variable debris locations, we can move beyond rigid interpretations of test results and embrace a more nuanced approach to diagnosing and treating BPPV. This subtle approach allows us to see beyond the surface and understand the complexities of vestibular disorders.
Key Takeaways:
Remember, the key to unraveling the mysteries of BPPV lies in understanding the specific symptoms and, more specifically, the signs (ie, nystagmus) a patient experiences. Dizziness demands clarity, and it's our job to delve deeper.
Recognize that BPPV can be more than just canals. It's a complex condition that can present unexpectedly, and we must be prepared for these variations.
Anatomical Interplay: Remember that vestibular tests can stimulate multiple canals.
Reid's Line Matters: Understand how the horizontal canal's angle influences nystagmus.
Debris is Dynamic: Understand that debris moves within the canals and that test results can be affected by the current location of the debris.
Conclusion:
This experience underscores the importance of thoroughly understanding vestibular anatomy and physiology. Clinical presentations can deviate from textbook descriptions, and we must be prepared to think critically and adapt our approach.
Call to Action:
Have you encountered similar BPPV presentations? Share your insights in the comments.
Subscribe for more vestibular rehabilitation knowledge.
Please share this article with your colleagues.