
Decoding the Dizziness-Anxiety Loop: Why Patients Get Functionally ‘Stuck’ in Maladaptive States
Clinical Review & Application of Multimodal Vestibular Therapy


The transition from an acute vestibular insult to chronic, functional dizziness is frequently driven not by peripheral failure, but by a persistent, maladaptive centralization of sensory processing. This “Maladaptive Vestibular Strategy” is a neurobiological state characterized by visual dependency, heightened vigilance, and behavioral avoidance. Evidence from recent systematic reviews (Ferlito et al., 2025) strongly indicates that breaking this self-perpetuating loop requires a multimodal intervention that simultaneously targets both the physical sensory mismatch and the psychological limbic response.
Introduction: The Neurology of Sensorimotor Mismatch
Chronic dizziness often outlasts the initial peripheral pathology (e.g., vestibular neuritis or BPPV). When patients fail to compensate centrally, the diagnosis frequently shifts to functional disorders such as Persistent Postural-Perceptual Dizziness (PPPD). The core pathophysiology is a persistent sensory mismatch.
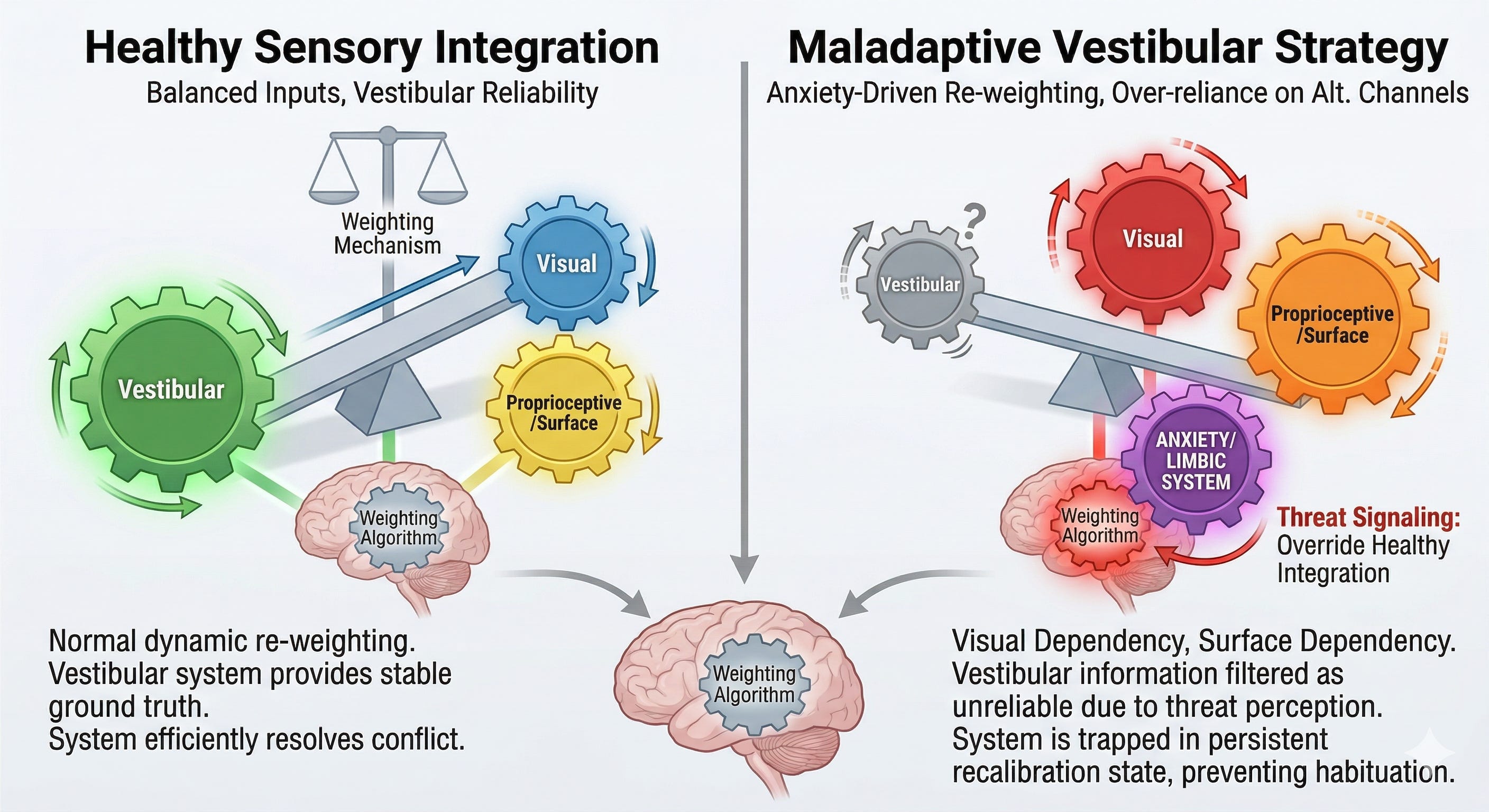
In a robust vestibular system, the brain resolves spatial orientation by cross-referencing vestibular, visual, and proprioceptive inputs. In functional dizziness, the brainstem’s “weighting algorithm”—the neural process that determines which sensory input to trust—becomes corrupted.
Instead of habituating and returning to dynamic equilibrium, the nervous system remains in a hyper-aroused, “threat-detection” mode. We must redefine our treatment goals from simple ‘habituation’ to a complete ‘facilitation of recalibration.’

Why Patients Get ‘Stuck’: The Role of Maladaptive Sensory Strategies
When vestibular information is perceived as unreliable (either due to acute insult or chronic over-vigilance), the limbic system signals a high-priority threat. The amygdala and the parabrachial nucleus activate the fear response, causing the patient to over-rely on alternative, stable sensory channels:
Visual Dependency: Over-weighting visual flow data. This leads to symptoms in visually complex environments (supermarkets, crowded streets) because normal retinal slip is misinterpreted as self-motion.
Surface Dependency: Over-weighting somatosensory feedback from the feet/surface. This causes excessive stiffness and a ‘high-guard’ gait.
These are maladaptive sensory strategies. They provide short-term stability but trap the patient in a self-perpetuating cycle. By ‘avoiding’ motion and triggers, the patient effectively starves the brain of the precise sensorimotor data required to coordinate correct re-weighting and optimize the vestibulo-ocular reflex. They are actively preventing the brain from learning that movement is safe.
Evidence-Based Recovery: The Case for Multimodal Therapy
We must aggressively target both the ‘fear’ and the ‘failure’ components of the loop.
A recent pivotal systematic review by Ferlito et al. (2025) examined the efficacy of integrating Vestibular Rehabilitation Therapy (VRT) with Cognitive Behavioral Therapy (CBT). The findings support a profound clinical shift:
“The efficacy of CBT in alleviating vestibular symptoms has been established... especially when the clinical condition is significantly influenced by comorbid anxiety and depression.” (Ferlito et al., 2025)
The study confirmed that combining VRT and CBT yields a synergistic effect, providing greater and more persistent reductions in dizziness-related handicap than either VRT or medication alone.
We must facilitate a precise internal signaling environment. In complex cases, we look to emerging research on mesenchymal signaling as a potential means of coordinating the biological microenvironment and supporting neural plasticity. Our goal is to optimize the system’s capacity to support the integrity of central compensation pathways. We cannot afford for these pathways to remain “stuck” in a state of threat.
Direct Clinical Implications for Practice
If your chronic vestibular patient is not improving with standard habituation/desensitization exercises, they are likely stuck in a maladaptive, anxiety-driven loop. Clinicians must shift their focus:
Identify Fear-Avoidance Early: Screen for visual dependence and catastrophic beliefs using tools such as the Dizziness Handicap Inventory (DHI) and the Catastrophizing Scale.
Integrate CBT Strategies: Do not just treat the balance; treat the brain’s perception of the threat to balance. Re-frame the vestibular mismatch as a non-catastrophic sensory error.
Encourage Exposure, Not Avoidance: Guide patients toward voluntary, progressive exposure to their triggers (optic flow, rapid head movement) in a controlled setting. We must facilitate the data collection that the brain needs to recalibrate.
Biological Signaling: Look beyond mechanics. Consider how we can actively coordinate the biological microenvironment to support neural repair and plasticity in severe, treatment-resistant cases. We aim to optimize the baseline physiological state to coordinate better outcomes.
Conclusion
Chronic functional dizziness is a disorder of centralized network processing, not peripheral failure. Breaking the loop requires an aggressive, multimodal approach that addresses the neurobiological sensory mismatch and the psychological avoidance. Clinicians must move beyond “coping strategies” and prioritize interventions that genuinely coordinate the re-establishment of dynamic sensory re-weighting.
Primary Clinical Reference:
Ferlito, S., et al. (2025). Anxiety-Related Functional Dizziness: A Systematic Review of the Recent Evidence on Vestibular, Cognitive Behavioral, and Integrative Therapies. Journal of Clinical Medicine, 14(2), 488. DOI: 10.3390/jcm14020488 / PMC12842955.
Agree and well penned. I just had a patient with the initial diagnosis of MdDS that did flip into PPPD. This was a challenging case for me and obviously the patient. Through some unconventional axial loading in clinic and home we successfully taught her brain that it was okay and safe not to sway, be dizzy and off balance. Four months later- she remains symptom free and has return to her normal lifestyle. Tenacity, thinking outside the box and consistency with her home VRT program were key!
If you are reading this and are being treated in VRT for MdDS- be encouraged!