

Ewald's Laws Demystified in Vestibular Science: A Deep Dive


Dizziness, vertigo, and balance disorders can be complex and frustrating for patients and practitioners alike. To navigate these conditions effectively, it's crucial to understand the vestibular system's underlying mechanisms. Ewald's laws, established over a century ago, provide a fundamental framework for understanding how the semicircular canals respond to head movement and generate specific nystagmus patterns.
The Three Laws: Beyond the Basics
Stimulation is Maximal in the Plane of the Canal:
Each semicircular canal is most sensitive to angular acceleration (head rotation) in its plane. The horizontal canals detect yaw (rotation around a vertical axis), the anterior canals detect pitch (nodding), and the posterior canals detect roll (tilting).
Ampullopetal Flow Excites the Horizontal Canal:
In the horizontal semicircular canals (HSC), movement of the endolymph (fluid) towards the ampulla (ampullopetal flow) increases the firing rate of the vestibulocochlear nerve (CN VIII). This excitation, processed in the vestibular nuclei, ultimately activates the abducens nerve (CN VI) and the oculomotor nerve (CN III), leading to eye movements in the same direction as the head rotation.
Ampullofugal Flow Excites the Vertical Canals:
In the posterior (PSC) and anterior (ASC) semicircular canals, movement of the endolymph away from the ampulla (ampullofugal flow) increases the firing rate of the vestibulocochlear nerve (CN VIII). This excitation, processed in the vestibular nuclei, activates the trochlear nerve (CN IV) and the oculomotor nerve (CN III), leading to torsional and vertical eye movements, respectively.
Ampullopetal vs. Ampullofugal Flow: The Mechanics
Ampullopetal: This term refers to endolymph flow towards the ampulla, a widened area at the base of each semicircular canal. This flow displaces the cupula (a gelatinous structure within the ampulla) in the short arm of the semicircular canal and bends the hair cells embedded within it, triggering nerve impulses in the vestibulocochlear nerve (CN VIII).
Ampullofugal: This term refers to endolymph flows away from the ampulla. The flow direction relative to the hair cells in the short arm of the semicircular canal determines whether the response is excitatory or inhibitory, again via the vestibulocochlear nerve (CN VIII).
Utriculopetal vs. Utriculofugal Flow: Otoconia Movement in BPPV
In the context of Benign Paroxysmal Positional Vertigo (BPPV), these terms describe the movement of otoconia (dislodged calcium carbonate crystals) within the short arm of the semicircular canals, specifically:
Utriculopetal Flow (Inhibitory in Vertical Canals): This refers to the movement of otoconia within the short arm of the posterior or anterior canal towards the utricle. This movement causes ampullopetal deflection of the cupula, leading to inhibition of the canal.
Utriculofugal Flow (Excitatory in Vertical Canals): This refers to the movement of otoconia within the short arm of the posterior or anterior canal away from the utricle. This movement causes ampullofugal deflection of the cupula, leading to excitation of the canal.
Hair Cell Orientation: The Key to Excitation and Inhibition
The orientation of hair cells within the sensory organs determines whether a particular direction of movement (ampullopetal/ampullofugal) will be excitatory or inhibitory.
Semicircular Canals: Hair cells are arranged in a specific orientation within the ampullae. In the horizontal canals, ampullopetal flow bends the hair cells towards their taller stereocilia, leading to excitation. In the vertical canals, the opposite is true – ampullofugal flow causes excitation.
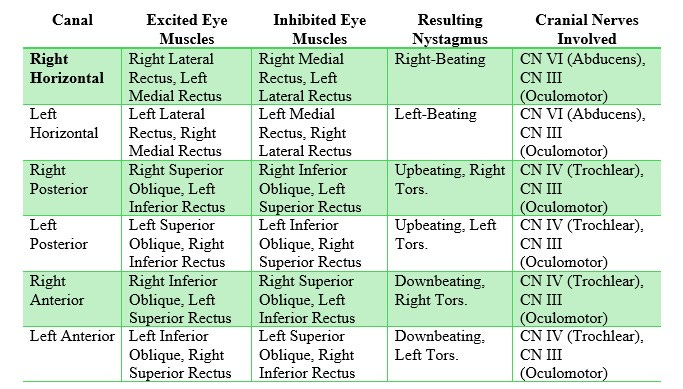
Canal Position, Eye Muscle Innervation, and Cranial Nerves
Each semicircular canal is connected to specific extraocular muscles via the vestibular nuclei and the medial longitudinal fasciculus (MLF). The vestibulocochlear nerve (CN VIII) carries sensory information from the vestibular organs to the brainstem. The specific cranial nerves responsible for the activation of the extraocular muscles are as follows:
Clinical Implications for Therapists
Understanding Ewald's Laws, hair cell orientation, the vestibulocochlear nerve (CN VIII), and the specific neural connections (including the cranial nerves) between the vestibular organs and eye muscles is essential for:
Accurate Diagnosis: Pinpointing the specific vestibular structure involved in a patient's dizziness or balance disorder.
Targeted Treatment: Designing effective treatment plans, including canalith repositioning maneuvers (e.g., Epley, Semont) for BPPV, vestibular rehabilitation exercises, and patient education.
Improved Outcomes: Enhancing patient outcomes by addressing the root cause of vestibular dysfunction and promoting recovery.
By delving into the depths of Ewald's laws and vestibular anatomy and physiology intricacies, you can unlock a deeper understanding of the vestibular system and its clinical implications. This knowledge empowers you to provide more precise and effective care for patients with dizziness, vertigo, and balance disorders.