
Is the Psychiatric Model Managing Illness or Manufacturing Customers in Vestibular Disease?

The critique of modern psychiatric models highlights a growing divide between traditional symptom-based management and the pursuit of true clinical resolution. In the article “Psychiatry’s Business Model, Manage the Symptoms, Keep the Customer Forever” (Illuminate The Illusion, 2026), the author exposes a staggering reality:
“The current system often lacks the financial incentive to actually heal patients.”
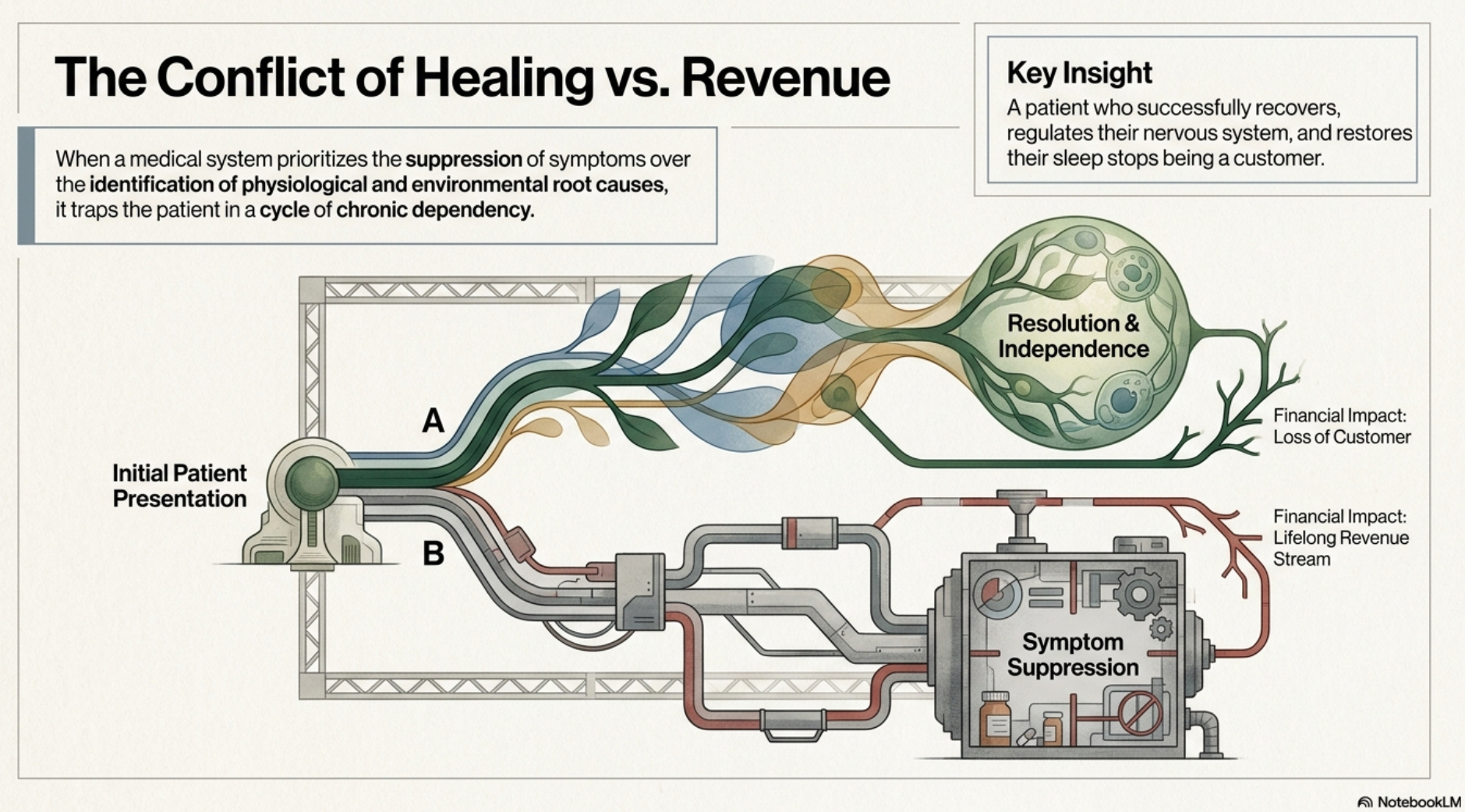
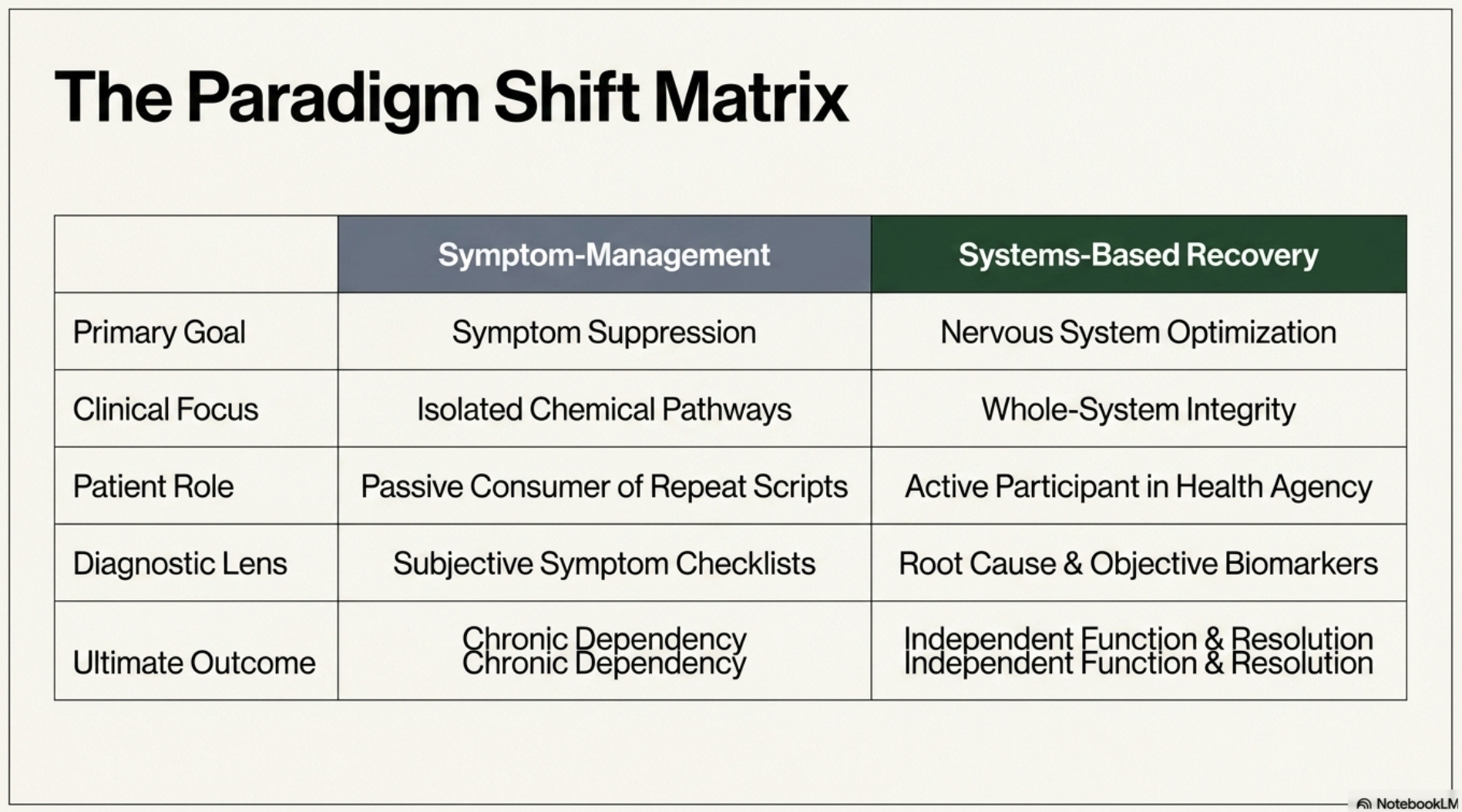
When a medical system prioritizes the suppression of symptoms over the identification of physiological and environmental root causes, it creates a cycle of “chronic dependency.”
This paradigm shift is particularly relevant to vestibular and neurological rehabilitation, where the goal must be to optimize the nervous system and facilitate the return to independent function.
Why Does the Symptom-Management Model Fail the Patient?
The author of the Illuminate The Illusion piece argues that a patient who recovers, regulates their nervous system, and restores their sleep stops being a customer. Chronic patients, however, represent lifelong revenue streams. This approach often relies on diagnostic frameworks that lack objective biological markers. By labeling a normal physiological response to trauma, environmental stress, or nutritional deficiency as a permanent disorder, the system effectively ignores the underlying somatic and sensory triggers.
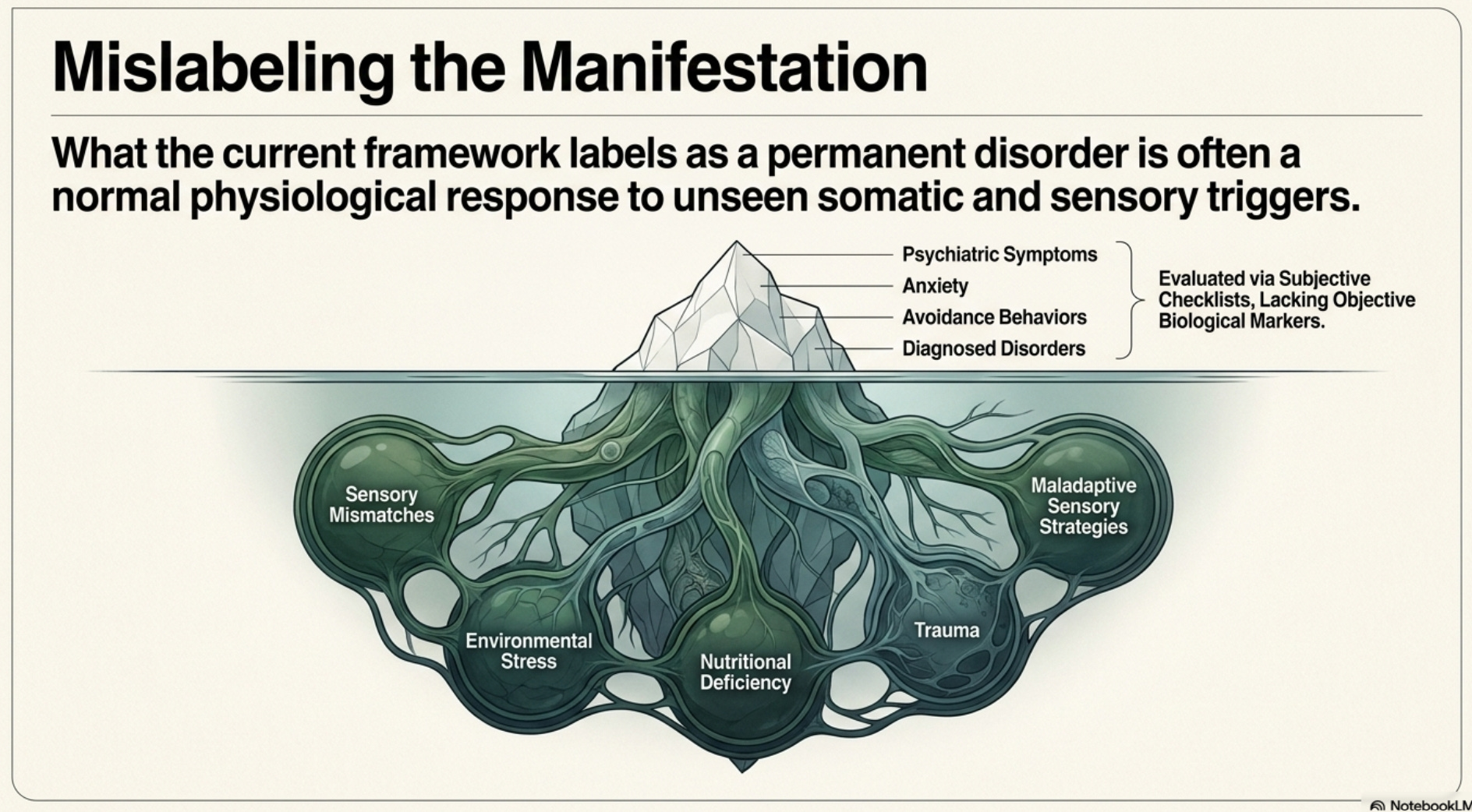
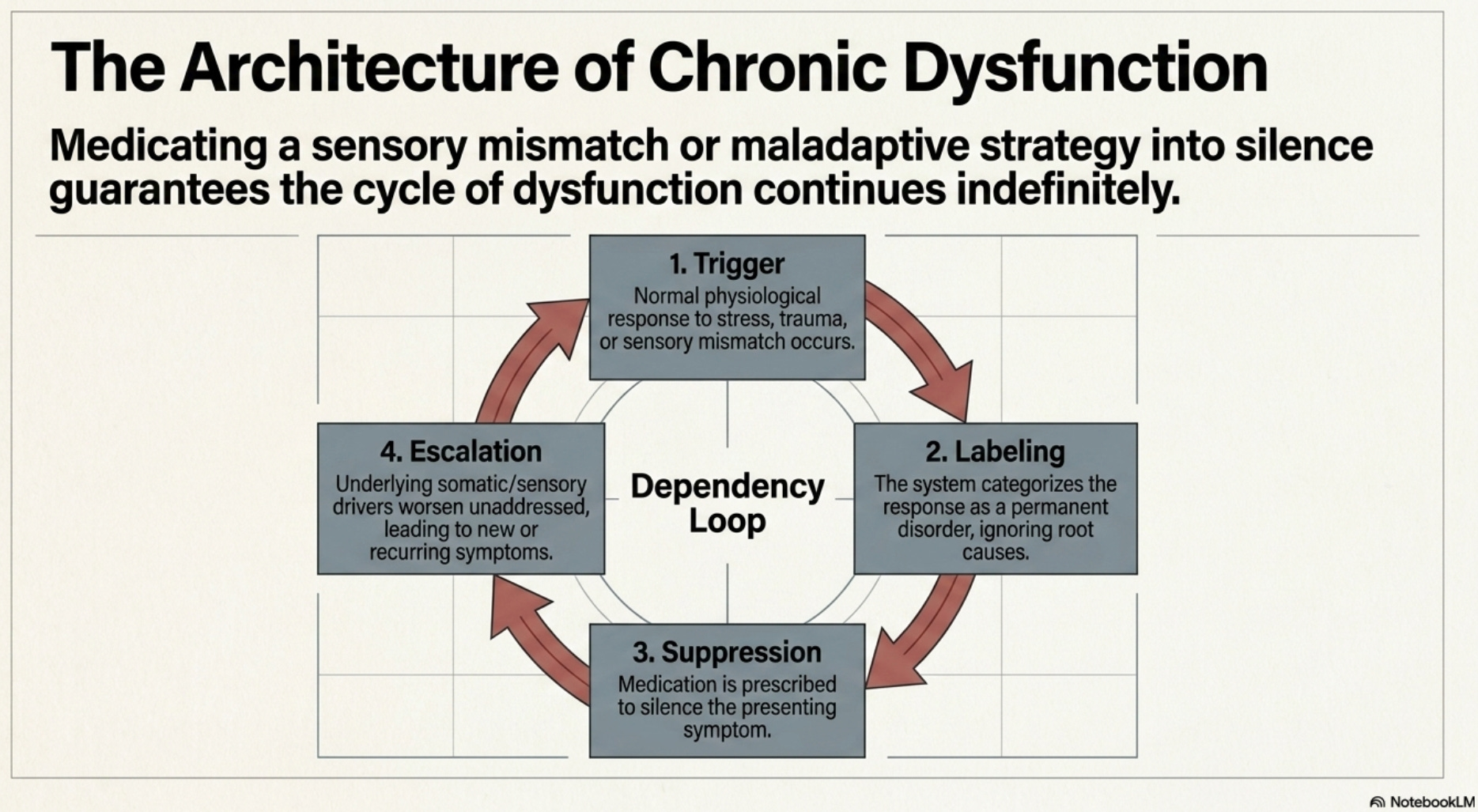
In many cases, what is labeled as a psychiatric symptom is actually a manifestation of a sensory mismatch or a maladaptive sensory strategy. When these issues are medicated into silence rather than addressed through targeted intervention, the patient remains trapped in a state of chronic dysfunction.
What Defines a Systems-Based Approach to Recovery?
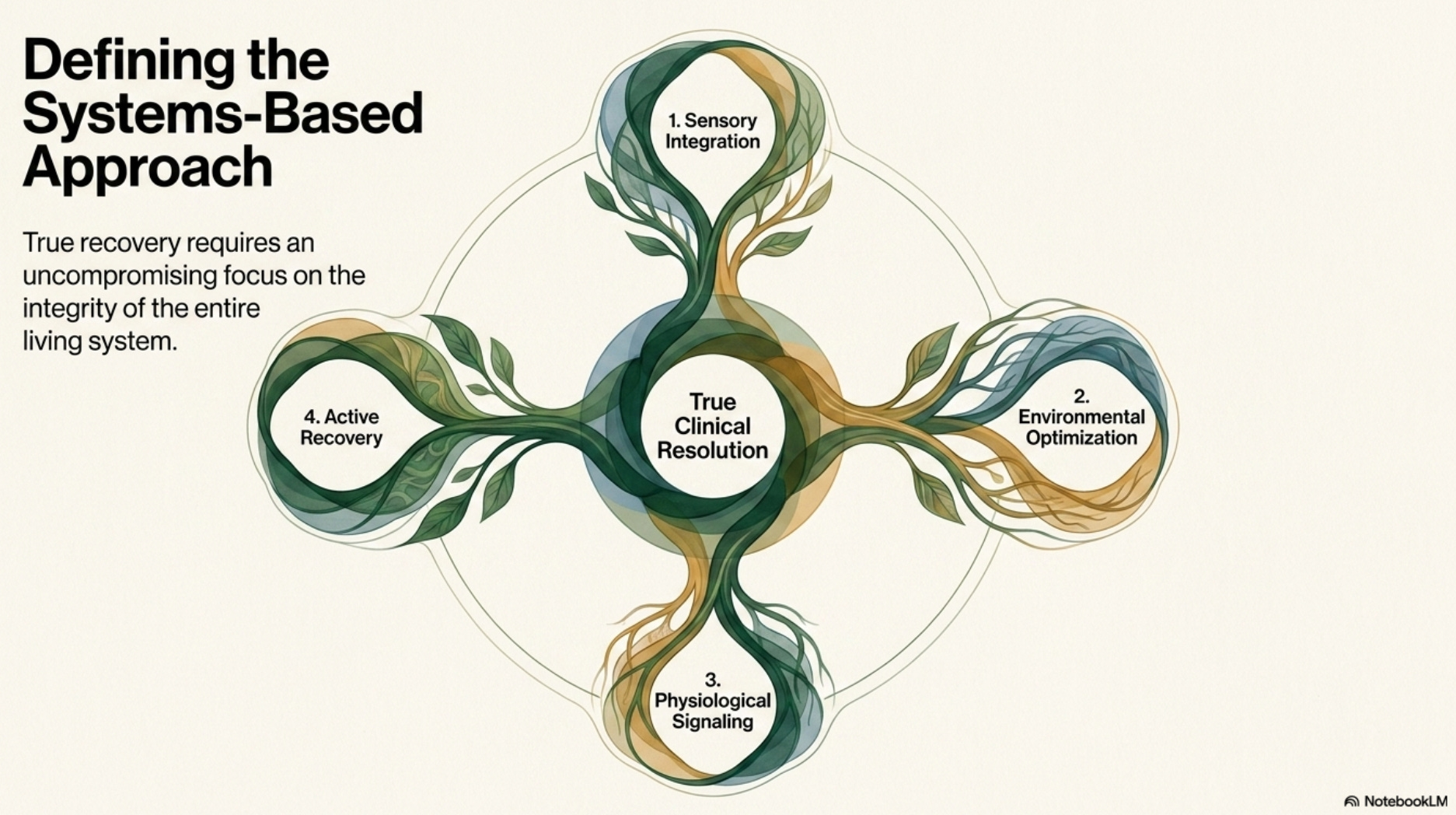
A systems-based approach recognizes that human suffering is rarely confined to a single chemical pathway. True recovery requires a focus on the integrity of the entire living system.
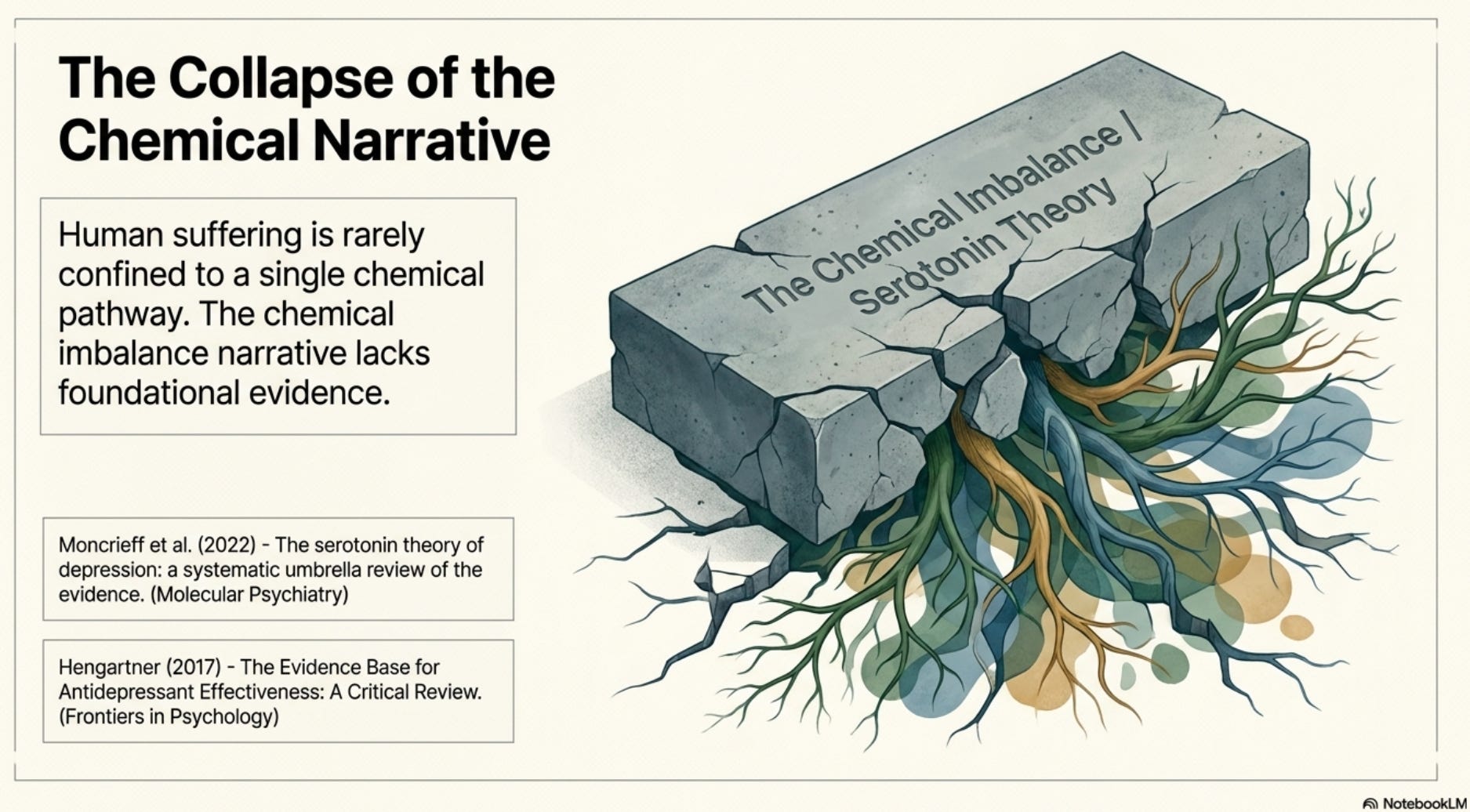
We must move away from “chemical imbalance” narratives that lack evidence and instead focus on:
Sensory Integration: Addressing a strong visual component or a strong somatosensory component that may be driving anxiety or avoidance behaviors.
Environmental Optimization: Identifying and modifying external factors, such as light, sound, and relational stress, that contribute to nervous system dysregulation.
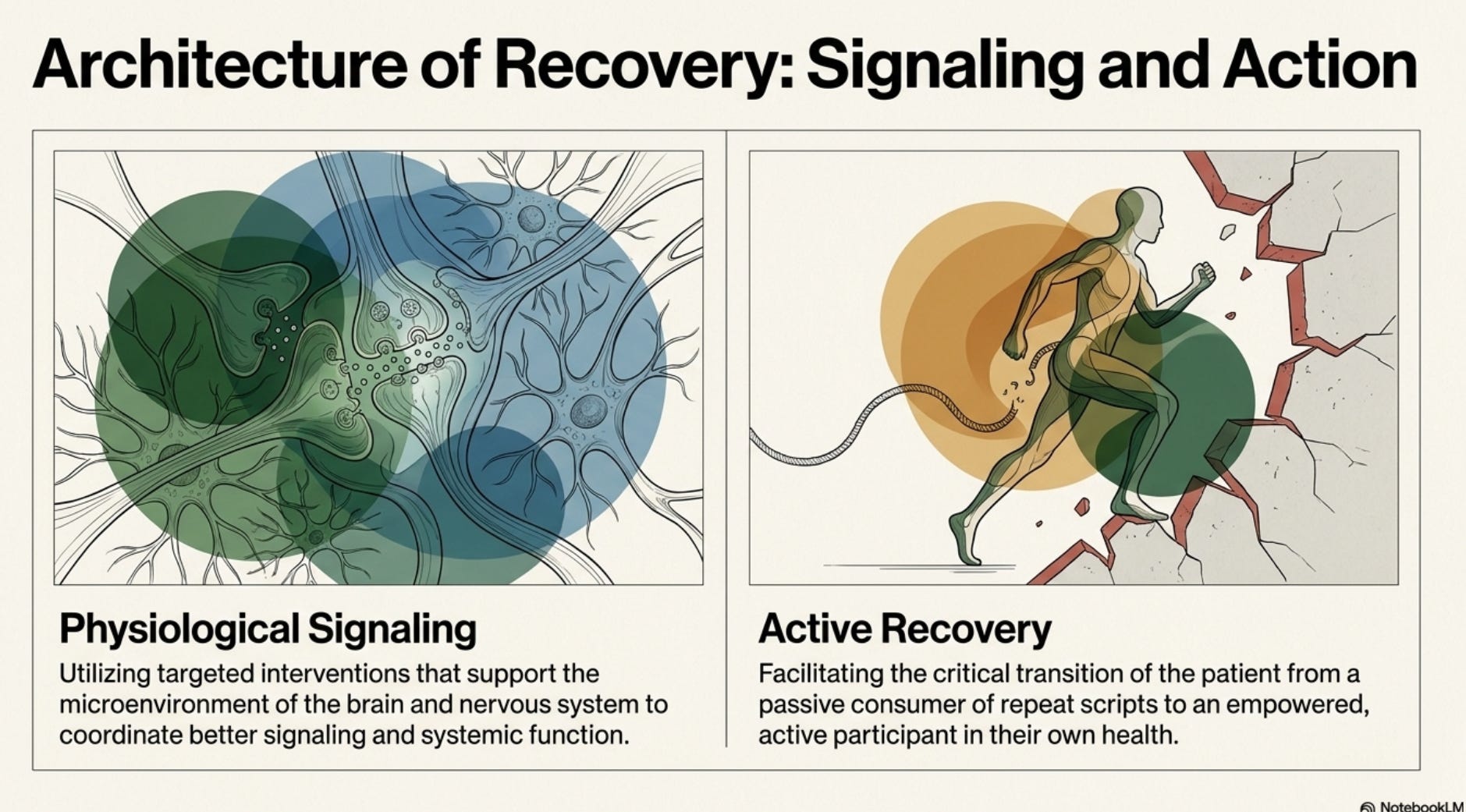
Physiological Signaling: Use interventions that support the microenvironment of the brain and nervous system to coordinate better signaling and function.
Active Recovery: Moving away from the role of a passive consumer of “repeat scripts” and toward an active participant in one’s own health.
Is It Time for Radical Honesty in Medicine?
The demand for transparency regarding the limitations of current diagnostic models is not “anti-science”; it is the foundation of ethical practice.
Real medicine must prioritize the mandate: “If in doubt, do nothing (do no harm).”
This requires an honest acknowledgment of iatrogenic injuries—damage caused by the treatment itself, including metabolic destruction and neurological injury—and a commitment to hunting for root causes rather than settling for lifelong management.
To improve the future of patient care, the focus must shift from “managing the illness” to “supporting the individual.” Professionals must be willing to look beyond the symptom checklists and address the complex, relational, and environmental realities of the human experience.
This discussion was inspired by the article on the Illuminate The Illusion Substack, which you can read here:

Disclaimer: The information provided in this article is for educational and informational purposes only and is for the discussion of clinical concepts. I am a Physical Therapist, not a medical doctor. This content does not constitute medical advice, diagnosis, or treatment. You should not use this information to disregard professional medical advice or delay seeking it. I am not advising you to stop, change, or start any medication. Any adjustments to your medical management must be made in direct consultation with your prescribing physician. This discussion is intended to support and coordinate a better understanding of the nervous system and does not claim to repair or cure any specific disease.
Citations:
Moncrieff, J., Cooper, R. E., Stockmann, T., Amendola, S., Hengartner, M. P., & Horowitz, M. A. (2022). The serotonin theory of depression: a systematic umbrella review of the evidence. Molecular Psychiatry. PMID: 35854107. DOI: 10.1038/s41380-022-01661-0
Hengartner, M. P. (2017). The Evidence Base for Antidepressant Effectiveness: A Critical Review. Frontiers in Psychology. PMID: 28223954. DOI: 10.3389/fpsyg.2017.00067
Vestibular therapists do the same thing in a different way. Ask me more about that sometime. I'm feeling much better since I got of that cash flow wheel. You are part of the medical profession just as psychiatrists. Glass houses...
Thank you - this is what patients, including those with rare/less common conditions, have been saying for years. Psychiatrists used to be very helpful to people with numerous conditions when it comes to understanding which medications can help and which can harm but nowadays my local pharmacist is up to speed with these issues so I don't need to involve psychiatrists in my care any longer although my psychotherapist is fab and has undone some of the iatrogenic harm done to me by the sloppy neuropsychiatrist I encountered at 'the sleep clinic' many years ago.
It's also worth noting that 'first, do no harm' is not part of the Hippocratic Oath (which many doctors don't take, these days). It reads 'if in doubt, do nothing'.
However 'psychiatric' and 'functional' (whatever that means on any given day of the week) still form part of the overarching vestibular conditions diagnostic Venn diagram which I think was created by Prof Staab. Hmm.