
Nystagmus Reversal in Infrared Video-Oculography (IVOG) Goggles: Ewald’s Law and the Observer’s Dilemma


This article proved to be one of the most challenging documents I have ever written. For eight hours, I battled the information pulled from the literature against the clinical reality I observe every day. The literature often presents the physiological truth, but the observer’s eyes see a reversed clinical reality. This internal conflict—where the technical physiological truth conflicts with the visual observation—is the exact reason practitioners get stuck. My experience suggests that the solution must align with what we observe to ensure accurate diagnosis and treatment.
Because this conflict is so persistent, I invite every vestibular specialist reading this—whether you are part of FYZICAL or practice anywhere else in the world—to review this article. Let us discuss this issue and agree on the best way to describe these movements for the next generation of therapists.
Introduction
I recall attending Susan Herdman’s Certification Course and sitting in the audience alongside approximately 500 other people. We were all staring at the massive screens on the walls that were part of the final test of our knowledge of vestibular pathologies. What they did was project eye movements onto the screens, and I recall one aspect that would throw people off was the fact that the eye movements were theoretically reversed. They were not projecting eye movements like our own; they were backwards. This eye movement ‘reversal’ is where many people failed the Herdman Course because they were unable to achieve the reversal. They kept thinking the right side was the right side and the left side was the left side of their own body, but did not realize that this anatomical situation was like looking in a mirror.
The Crucial ‘Crossing Over’ Principle
To become proficient, you must understand this key principle. The reversal of the image on the screen works just like a handshake. When you reach out your right hand, you meet the other person’s right hand, reaching across your body. The same principle applies to the patient in front of you. When you look at their eyes on the screen, your right side aligns with the patient’s left side, and your left side with their right. This anatomical reversal is why you must account for this ‘crossing over’ to interpret horizontal and torsional movements correctly.
Decoding the Directions: A Clinical Breakdown
Only two of the three planes of eye movement reverse when you look at them through the goggles. Misinterpreting the reversal of these two planes can lead you down a completely inappropriate diagnostic and treatment path.
Horizontal: The horizontal movement is the one that mirrors. A nystagmus that appears to have its fast phase beating to the left on the screen is actually a ‘right-beating nystagmus’ from the patient’s perspective. This means the quick correction moves toward the patient’s right ear. If you misinterpret this movement, you are on the wrong path entirely.
Vertical: The vertical movement is straightforward. What appears as a ‘down-beating nystagmus’ on the screen is an actual ‘down-beating nystagmus’. It is not reversed. The quick phase moves inferiorly, and a glance at the goggles is all you need to determine this vertical direction.

Torsional: The torsional component also reverses. The visual movement you see on the screen is what you must observe. A typical example is right posterior semicircular canal BPPV, which typically presents with a classic Dix-Hallpike test characterized by an upbeat and torsional nystagmus to the right. Misinterpreting this torsional movement can lead to performing an inappropriate repositioning maneuver on the incorrect side.
The Foundation: Ewald’s First Law and the Vestibular Response
To truly understand the movement of the eye, you must understand a few fundamental rules, starting with Ewald’s First Law. This law states that the plane of the semicircular canal determines the plane of the nystagmus response. In other words, when you stimulate a specific canal, the eye movement you observe occurs in the exact plane of that particular canal.
This concept is the most critical part: Ewald correctly described the slow phase of the nystagmus as the ‘vestibular response’. This slow, methodical movement is the direct result of the vestibular system trying to compensate for a head movement or stimulus. The fast phase is a corrective, or repositioning, saccade that the brain performs to recenter the eye.

To truly understand the vestibular response, it is essential to consider the mechanisms of pushing and pulling. When you excite one canal, it creates a ‘pushing’ force on the eye. Simultaneously, you inhibit the contralateral canal, which creates a ‘pulling’ force. This coordinated push-pull movement is the slow phase of the movement.
For example, when you turn your head to the right, your eyes move slowly to the left. This slow, smooth movement to the left is the vestibular response. The quick movement of the eye back to the right is the brain’s corrective saccade. We identify nystagmus by its fast phase, but the slow phase tells us what the vestibular system does.
If you are listening to this article, you must stop for a moment. Look at the chart. Make sure you understand the table clearly. The directions in this table reflect the appearance of the eye movement on the practitioner’s video screen (with the torsional reversal applied).
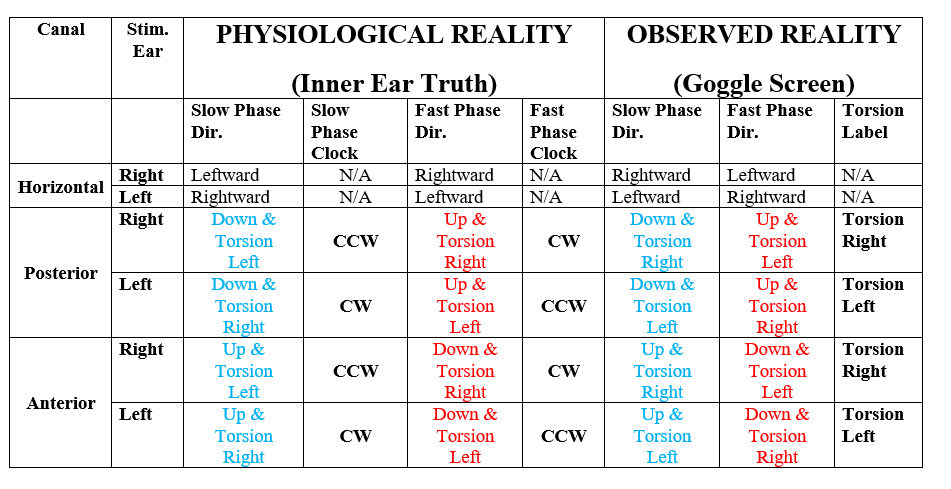
Understanding this table and identifying both the vestibular slow phase and the corrective fast phase is essential for making a correct diagnosis. Without this knowledge, we are merely guessing at the true nature of the underlying problem.
Resolving the Torsional Conflict on Screen: The Visual Truth
Many practitioners confuse the torsional movement because they attempt to reverse-engineer the nystagmus back to the patient’s actual physiology before they label the movement. Stop this action immediately. You must prioritize the visual output from the goggles. This is what you see, and this is what you label.
- You must label the visual output from the goggles - Asprella-Libonati - 2012Here is the simple breakdown for the Fast Phase of the Right Posterior Canal (RPC), which is the most commonly confusing scenario:
Patient’s Physiological Reality: The actual nystagmus is Upbeat and ‘Clockwise (CW)’. This is the truth of the inner ear.
Practitioner’s Visual Observation (The Goggle Reversal): You observe the Upbeat component clearly. The goggle’s mirror effect reverses the torsional element. This reversal causes the actual ‘Clockwise’ rotation to appear visually as ‘Counterclockwise’ rotation on your screen, which you label as Torsion Right.
The Simple Rule: What You See Is What You Label. The easiest and most reliable way to avoid error is to simply write what you see (Upbeat and Torsion Right) and stay away from using clockwise and counterclockwise in your clinical notes. Why? Because physiologically, both terms are technically correct depending on the viewpoint, and that confusion is exactly what derails accurate documentation. You must label the Torsion Right or Torsion Left that you directly observe on the screen.
This precise mechanism mandates that you describe what you see on the screen: Upbeat and Torsion Right. This relationship is non-negotiable and represents the most crucial step in correctly interpreting the video feed.
The image above is the ultimate visual validation. It demonstrates that when the eyes are rotated Clockwise (CW) physiologically, the reversed image on the monitor shows the torsional component as Counterclockwise (CCW), leading to the clinical label of ‘Torsion Right.’ You are witnessing the reversal, and you must identify it. If you attempt to skip this step, you will be wrong.
Why This Simple Detail is Critical
Getting these reversals and the correct vestibular responses right is crucial for making accurate assessments and developing effective treatment plans. This small detail can completely alter a diagnosis, which is why it is one of the primary reasons people have failed to obtain their certification. You cannot fly by the seat of your pants in vestibular therapy. This simple piece of information is a key step in decoding a patient’s clinical presentation.