
Oculomotor Dysfunction: Why Assessing Vergence and Phorias is Crucial in Concussion and Vestibular Therapy


Vergence, the simultaneous movement of the eyes in opposite directions, is a vital part of the visual system. It allows us to maintain a single, clear vision as we shift our gaze from far to near. In the context of vestibular and balance rehabilitation, dysfunction in this oculomotor system can severely impact a patient’s recovery from a concussion or a vestibular disorder, directly affecting their balance and provoking dizziness. Therefore, physical therapists must accurately assess and address vergence dysfunctions and underlying deviations to achieve optimal patient outcomes.
Key Terminology
Phoria: A latent (hidden) deviation of the eye that is only revealed when fusion (binocular viewing) is intentionally broken (e.g., during the Cross-Cover Test).
Tropia: A manifest (always present) deviation of the eye; the eye is visibly turned even during binocular viewing.
Esophoria: A latent inward deviation of the eye (toward the nose).
Exophoria: A latent outward deviation of the eye (away from the nose).
Fusional Reserve: The amount of vergence (inward or outward) a person can use to maintain single vision.
The Four Components That Drive Vergence
The oculomotor system uses four distinct components to generate the complete vergence response, ensuring stable, singular vision.
Tonic Vergence: This component sets the physiological position of rest, which determines the baseline alignment of the eyes. This resting position, known as a phoria or a tropia, influences the starting point for all other vergence movements.
Proximal Vergence (NPC): This acts as a course adjustment, initiating a significant shift in eye position when a person changes their focus (gaze) from Distance to near.
Accommodative Vergence: As we focus on a near object, our eyes accommodate (change focus), and this act automatically drives a related change in vergence.
Fusional Vergence (Disparity): This component provides the fine adjustment. It holds and corresponds to small changes in visual disparity, actively maintaining binocular alignment.
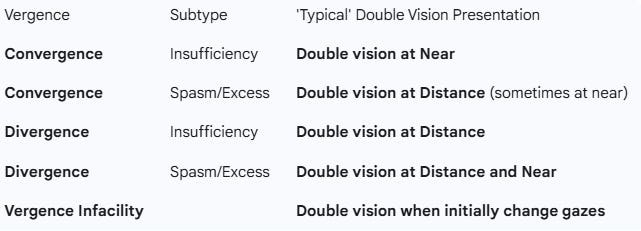
Understanding Vergence Dysfunctions
Failure to address these dysfunctions can lead to persistent symptoms, prolonged recovery, and decreased patient satisfaction. Dysfunction in these components can lead to diplopia (double vision) and difficulty with dynamic balance. If you are listening, take a minute to review the chart.
Clinical Pearl: Assessing Phorias with the Cross-Cover Test
In concussion and post-concussion syndrome, oculomotor impairments, especially vergence dysfunctions, are among the most common and persistent findings. However, a specialized assessment for underlying deviations, such as the Cross-Cover Test, is an essential strabismus pearl that dictates the safety of treatment.

The Cross-Cover Test (also known as the Alternating Cover Test) is the crucial assessment that breaks fusion and reveals the full extent of the tonic vergence deviation (phoria).
Physical therapists must exercise extreme care when this test reveals a significant, pronounced phoric eye movement, whether esophoric or exophoric.
A key strabismus pearl, emphasized by experts like developmental optometrist Dr. Jacqueline Theis, OD, is this:
‘If you see a patient with a big eye turn, and they do not see double, leave it alone.’
This significant deviation is a stable, long-term adaptation. The patient’s brain has suppressed or compensated for this alignment issue. Applying inappropriate training can overwhelm the patient’s fusional reserves, destabilize their vision, and create a new, debilitating visual problem that causes increased dizziness and headaches.
Therefore, simple vergence training, such as pencil push-ups or Brock string exercises, is strongly discouraged in the presence of a large, non-symptomatic phoria. This treatment is outside the physical therapist’s scope. If a large phoria or any manifest tropia is identified, the therapist must prioritize referral to a developmental optometrist or neuro-optometrist. These specialists can provide appropriate compensatory treatment, such as prisms or lenses, which often stabilizes the visual system and allows the patient to engage in targeted physical therapy successfully.
Targeted Vestibular and Oculomotor Therapy
Once any underlying stability issues are addressed, the rehabilitation program focuses on targeted visual-vestibular exercises. These exercises train the patient’s brain to reestablish connections between the visual, vestibular, and somatosensory inputs. The goal is to reestablish the automatic, subconscious control of eye movements, which is the final key to restoring stable vision and confident balance. By integrating these oculomotor assessments, applying the appropriate clinical cautions, and using targeted treatments, therapists can significantly improve patient outcomes and quality of life.
Brian Werner, PT, MPT, is a physical therapist who has been specializing in vestibular and balance disorders for over a quarter of a century. He is the founder of the FYZICAL Balance Paradigm and one of the co-founders of FYZICAL, LLC, Balance Center Division with Dr. Daniel Deems, MD, PhD, where he serves as the National Director of Vestibular Education & Training. His extensive experience and contributions to the field make him a trusted authority on this topic.