

Part 3: Semicircular Canal Anatomy: A Crucial Aspect for Vestibular Professionals


The semicircular canals are not just interesting anatomical structures but essential components of the vestibular system. They sense angular acceleration and contribute to our sense of balance and spatial orientation. As vestibular professionals, thoroughly understanding their anatomy is crucial to diagnosing and treating balance disorders.
The Three Canals
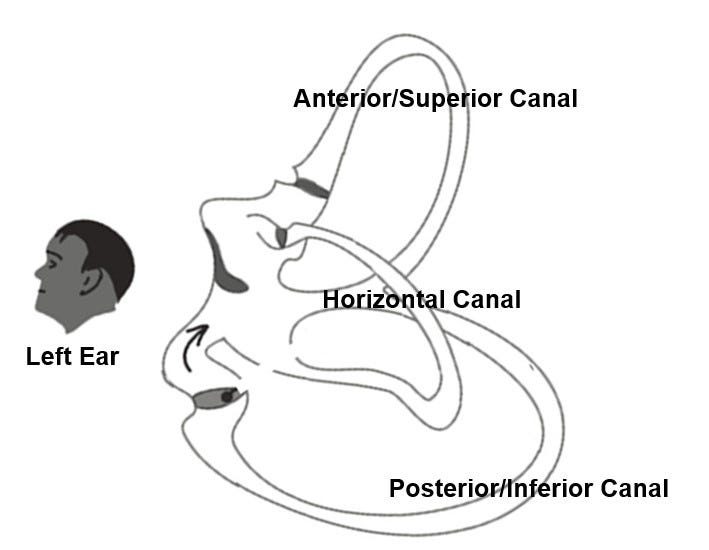
The vestibular system contains three semicircular canals, each oriented orthogonally to the others:
Anterior/Superior Canal: Detects movement in the sagittal plane (e.g., nodding "yes").
Posterior/Inferior Canal: Detects movement in the coronal plane (e.g., tilting the head side to side).
Lateral/Horizontal Canal: This canal detects movement in the horizontal plane (e.g., shaking the head "no").
Long and Short Arms: Clarifying the Anatomy
A long arm and a short arm characterize each semicircular canal.
Short Arm (SA): This segment directly connects the ampulla to the utricle, a structure within the vestibule that responds to linear acceleration and head tilt.
Long Arm (LA): This arm extends from the ampulla and houses two distinct segments:
Anterior Arm (AA - Ampullary Segment): This segment contains the ampulla, an expanded region housing the sensory receptor cells (hair cells) embedded within a gelatinous mass called the cupula. Deflection of the cupula during angular head movements stimulates the hair cells, initiating the transduction of the mechanical stimulus into neural signals.
Posterior Arm (PA - Non-ampullary Segment): This segment connects the ampulla to the common crus (for the anterior and posterior canals) or directly to the vestibule (for the lateral canal).
Intermediate Segment: This segment represents the semicircular canal's curved portion, connecting the extended arm's anterior and posterior arms.
Functional Significance and Clinical Relevance
This division into anterior and posterior arms within the long arm is critical for the push-pull dynamic of the semicircular canals. The endolymph fluid within the corresponding canal lags due to inertia when the head rotates in a specific plane. This lag deflects the cupula within the ampulla, exciting the hair cells on one side and inhibiting those on the other. This mechanism allows for precise detection of head rotation direction and velocity.
Furthermore, this detailed anatomical knowledge is theoretical and crucial for understanding and managing vestibular disorders. For instance, in benign paroxysmal positional vertigo (BPPV), debris (otoconia) becomes dislodged and migrates into a semicircular canal. By accurately identifying the location of the debris – whether it's in the anterior arm, posterior arm, or intermediate segment – clinicians can select the most appropriate canalith repositioning maneuver to treat the condition effectively.
Understanding the intricate anatomy of the semicircular canals, including the distinction between long and short arms and the functional segments within, provides vestibular professionals with a solid foundation for accurate assessment and effective management of patients with balance disorders. This knowledge is not just theoretical, but it directly impacts the quality of care we can provide to our patients, helping us to accurately diagnose and effectively treat their conditions, thereby improving their quality of life.
I would say looking at the variations in head sizes and shapes, I am sure there are a lot.
Great work! How often do you think there are anatomical anomalies with our patients? I feel like it is frequent with the tough rebellious cases, but not sure if I'm just making excuses for not understanding why some of my patients don't get better as quickly as I would like.