
Part Two: Reverse Engineering the High-Gain Brain—The Path to Integration

In Part One, we established the physiological foundation of Visual Snow Syndrome (VSS) as a state of thalamocortical dysrhythmia. For the vestibular professional, understanding the ‘why’ is only the prelude. To effectively coordinate a treatment plan that significantly improves patients' outcomes, we must reverse-engineer the maladaptive strategies the nervous system adopts to survive ‘noise.’ Our goal is to convert this neural insight into a step-by-step treatment roadmap.
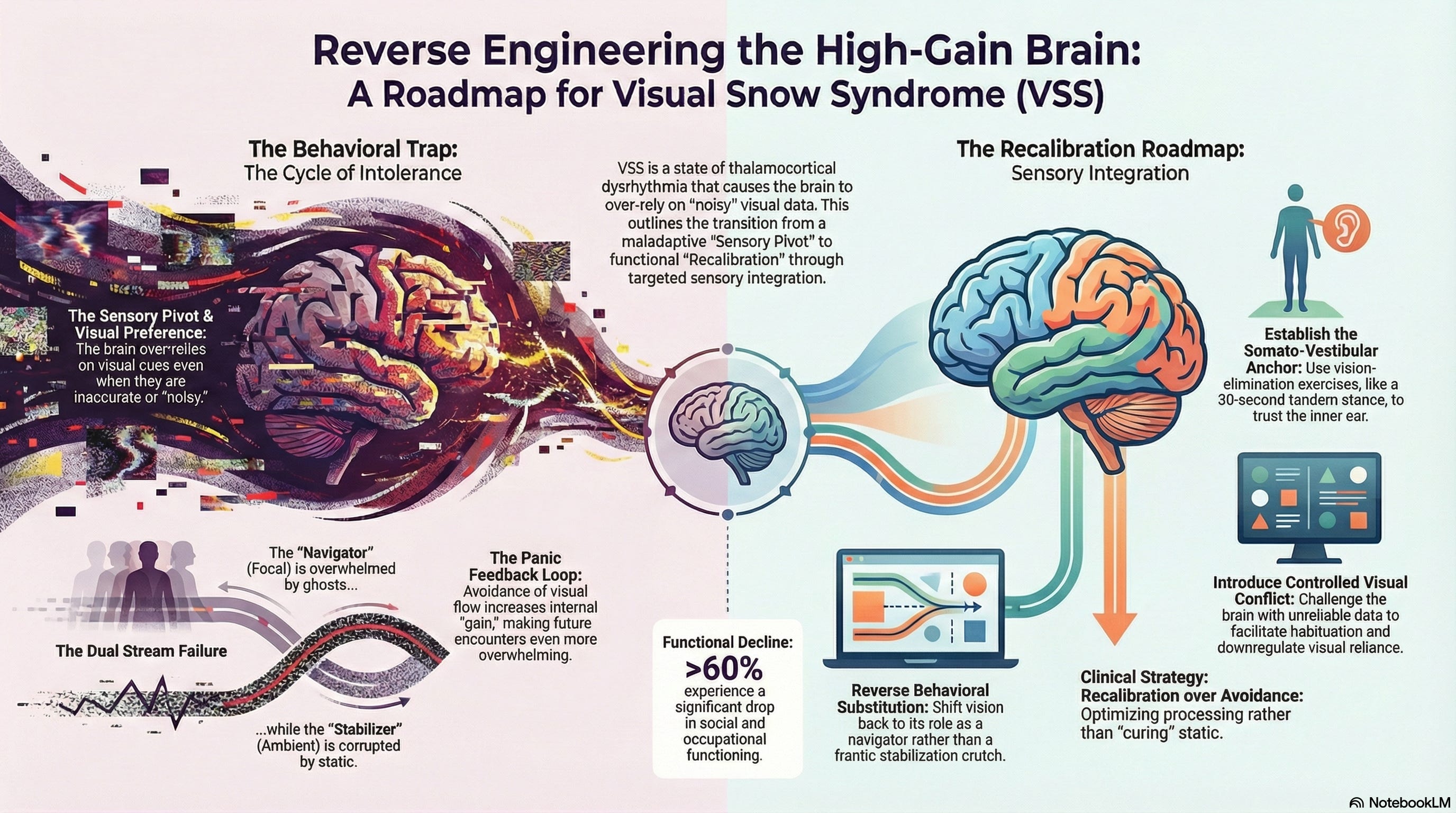
The Behavioral Trap: Identifying the Sensory Pivot
To begin the reverse-engineering process, we must first identify the behaviors the patient uses to avoid symptoms. VSS rarely remains a stagnant visual nuisance; it evolves into a pervasive, maladaptive sensory strategy.
When the brain is inundated with ‘noisy’ visual data, a ‘sensory pivot’ occurs. The patient naturally develops avoidance behaviors that eventually become a self-reinforcing loop. The literature in vestibular science confirms that chronic sensory conflict leads to ‘visual preference’, in which the brain overrelies on visual cues even when they are inaccurate (Pavlou et al., 2011).
Visual Avoidance: The patient avoids environments with high visual flow (e.g., stores, driving, screens).
Intolerance Cycle: This avoidance prevents natural habituation. The brain, starved of healthy data, increases its internal ‘gain’ to scan for threats, making the next visual encounter even more overwhelming.
The Panic Feedback Loop: This state of ‘visual vertigo’ or ‘VVM’ (Visual-Vestibular Mismatch) induces high autonomic arousal (Bronstein, 1995).
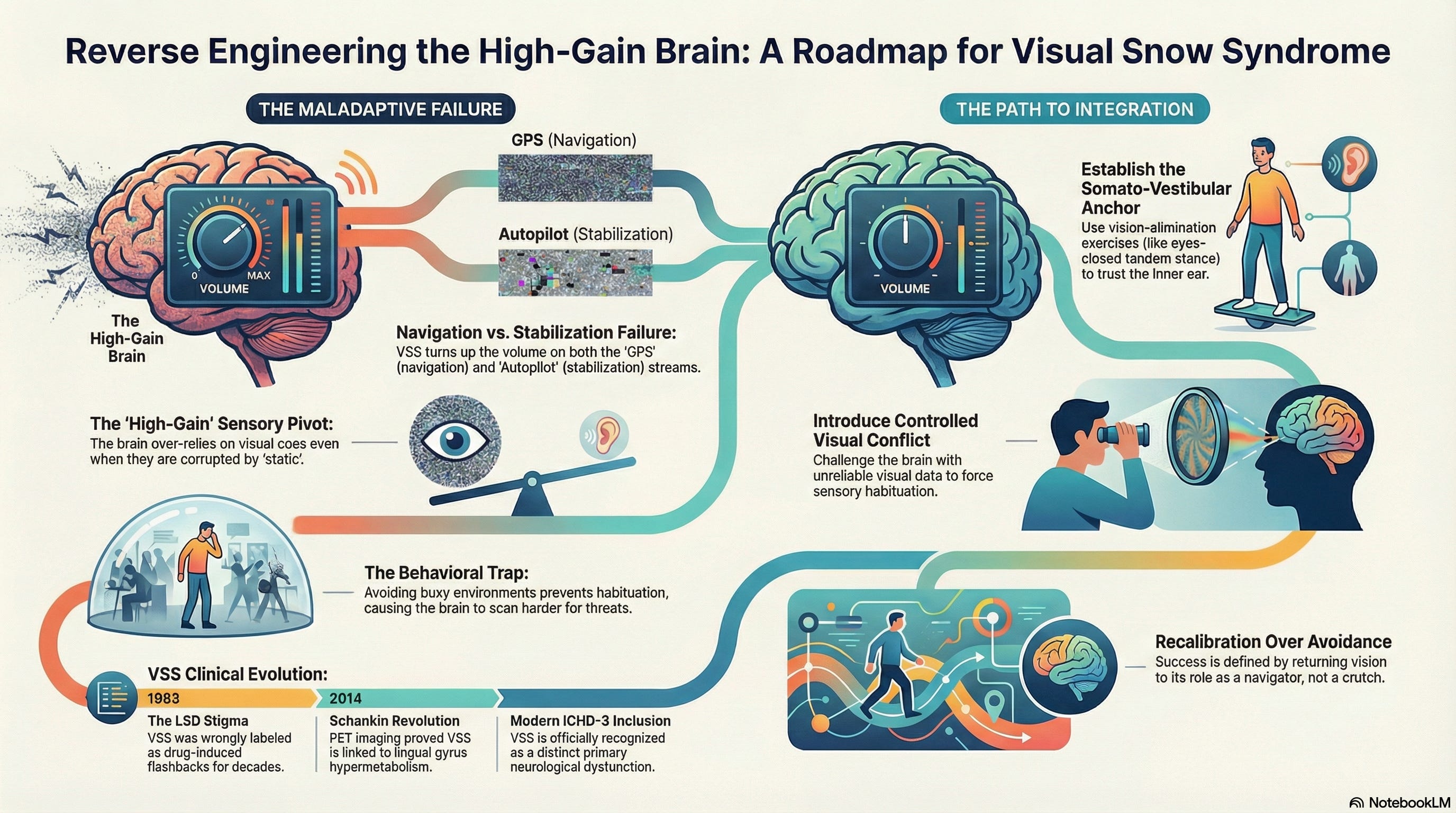
The Dual Failure: Navigation vs. Stabilization
In a healthy system, vision functions through two distinct streams: the Ambient, akin to an autopilot that stabilizes, and the Focal, similar to a GPS that navigates. Normally, the ambient system remains quiet, effectively suppressing internal noise to ensure a stable horizon, while the focal system stays sharp, empowering us to identify objects and move through space efficiently. To clarify: In healthy vision, the ambient stream is quiet like a calm autopilot, and the focal stream is sharp like a precise GPS. However, in Visual Snow Syndrome, both streams are unusually loud, disrupting this natural balance.
In the ‘VSVM’ (Vision > Somatosensory + Vestibular Mismatch) profile, the brain is in a state of cortical hyperexcitability. It turns the gain up on both streams simultaneously, leading to a dual failure:
The Hypersensitive Navigator: The focal system becomes overwhelmed by ‘palinopsia’ (trailing images). The brain attempts to move forward, but the ‘ghosts’ of the previous visual frame slow processing. To engage in this understanding, consider the following: Which simple office task would reveal palinopsia to you today? This actionable prompt encourages immediate experimentation and learning by doing.
The Over-Active Stabilizer: Because the brain no longer trusts the vestibular system, it forces the ambient visual system to become the primary stabilizer. However, due to the ‘static’, the brain attempts to ‘balance’ off a signal that is constantly flickering.
The brain tries to stabilize using a corrupted signal, which only creates more perceived instability. To compensate, it further increases the surface radar volume, leading to the extreme surface dependence we observe in the clinic.
Advanced Sensory Organization Testing: Mapping the Mismatch
To address the challenges of treatment execution, we use Advanced Sensory Organization Testing (SOT). We are not just looking for balance; we are looking for how the brain has mapped its survival. We are looking for the ‘VVM’. Advanced SOT allows us to isolate the systems and identify if the patient is functioning with a maladaptive sensory strategy. These patients often show a profound inability to ignore inaccurate visual data (visual conflict) or maintain stability when the surface is compromised. In practice, this can be broken down into a quick checklist to facilitate implementation:
1. Does the patient insist on using visual cues in low-contrast environments, despite the availability of other sensory inputs?
2. Are there repeated observations of lost balance when the surface or environment changes unexpectedly?
3. Is there a reliance on visual reassurance when performing tasks, even simple ones?
They are ‘clinging’ to a faulty visual signal to control symptoms, but in the end, this strategy only makes them worse by increasing their intolerance to the world around them.
The Methodology: Recalibration over Avoidance
It is critical to understand that Sensory Integration Therapy is not a ‘cure.’ We are not fixing the underlying neurological static; rather, we are optimizing how the brain processes it. This approach offers a path to enhanced function, building a foundation for improved quality of life. By reframing treatment as an opportunity for growth and adaptation, we provide hope and maintain realistic expectations, nurturing both patient trust and motivation.
1. Establishing the Somato-Vestibular Anchor
We initiate the process by implementing vision-elimination exercises to encourage the brain to find a reliable anchor. A foundational exercise involves standing in a tandem stance with eyes closed for 30 seconds. This exercise tests the nervous system by removing visual cues, demonstrating to the brain that stability can be achieved without the ‘noisy’ visual stabilizer. This method helps restore trust in the feet and the inner ear.
2. Introducing Controlled Visual Conflict
Once the anchor is established, we introduce ‘visual conflict.’ By challenging the brain with unreliable visual data, we facilitate sensory habituation. This teaches the nervous system to downregulate its reliance on vision—effectively breaking the ‘VVM’ (Whitney et al., 2016).
3. Breaking the Maladaptive Substitution
As the patient learns to trust their body again, the ‘need’ to cling to the visual field for stability decreases. This is behavioral substitution in reverse. We support the brain’s return to using vision for navigation rather than as a frantic stabilization crutch.
Case Study: Reversing the Slippery Slope
Consider a 54-year-old female who lived with VSS for three years. She had fallen deep into the cycle of avoidance, housebound and unable to navigate a store or watch a television screen without intense symptoms and panic. She exhausted multiple traditional approaches before finding a physical therapist who understood sensory integration.
Through a slow, steady progression of exercises where the therapist provided a progressive framework of disengaging visual input, she was finally able to:
Navigate a grocery store.
Watch television comfortably for the first time in years.
Coordinate her movements in high-flow environments.
Optimize her sensory environment to reduce the autonomic panic response.
Conclusion: Making the Patient Better
The real challenge of VSS is the slippery slope of intolerance. If we do not reverse engineer the patient’s behaviors and address the ‘VVM’ mismatch through Advanced Sensory Organization Testing, their world will continue to shrink. Untreated, VSS can lead to a marked decline in quality of life, with studies indicating that over 60% of sufferers experience a significant drop in social and occupational functioning. It underscores the urgency of tackling the issue. While we are not ‘curing’ the disorder, by focusing on sensory integration therapy—specifically down-regulating visual sensitivity while supporting vestibular and somatosensory signaling—we can help patients regain their lives and feel significantly better.
References
Aeschlimann, M., Klein, A., & Schankin, C. J. (2024). Visual snow syndrome: A clinical and pathophysiological update. Journal of Clinical Medicine, 13(5), 1373. https://doi.org/10.3390/jcm13051373
Bronstein, A. M. (1995). Visual vertigo: Syndrome and mechanisms. Journal of Neurology, Neurosurgery & Psychiatry, 59(5), 472-476.
Ciuffreda, K. J., Tannen, B., Tannen, N., & Rutner, R. (2024). Visual snow syndrome: Therapeutic implications. Advances in Ophthalmology and Optometry, 9, 1–23. https://doi.org/10.1016/j.yaoo.2023.12.001
Horak, F. B. (2006). Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age and Ageing, 35(suppl_2), ii7-ii11.
Klein, A., & Schankin, C. J. (2021). Visual snow syndrome as a network disorder: A systematic review. Frontiers in Neurology, 12, 724072. https://doi.org/10.3389/fneur.2021.724072
Pavlou, M., et al. (2011). Visual vertigo and dizziness after images: The effects of visual stimulus complexity. Journal of Vestibular Research, 21(3), 145-156.
Whitney, S. L., et al. (2016). The utility of the dizziness handicap inventory and the sensory organization test in patients with visual vertigo. Journal of Vestibular Research.
White, O. B., et al. (2022). Editorial: Visual snow: Old problem, new understanding. Frontiers in Neurology, 13, 884752.