


Why physicians and rehabilitation therapists look at the exact same concussion through two fundamentally different diagnostic lenses.
Clinical Outcome Measures for Concussion:
Clinicians evaluate mild traumatic brain injury recovery using standardized self-report tools that quantify symptom volume and severity. Selecting the proper assessment scale allows the care team to differentiate between acute sports-related physiological changes and long-term neurofunctional impairments.
A persistent operational divide exists within multi-disciplinary concussion clinics regarding self-report outcome measures. Physicians routinely favor the Post-Concussion Symptom Scale (PCSS) to guide medical clearance, while physical, occupational, and speech therapists frequently employ the Rivermead Post-Concussion Symptoms Questionnaire (RPQ). This division stems from differing diagnostic priorities rather than a lack of standardized consensus.
Why Do Physicians Prefer the Post-Concussion Symptom Scale?
Medical doctors choose the PCSS because the tool integrates directly into acute sports medicine clearance protocols and yields high numerical resolution across the immediate recovery timeline. The instrument comprises 22 distinct items on a 0-6 Likert severity scale, capturing subtle fluctuations in the brain's systemic metabolic distress.
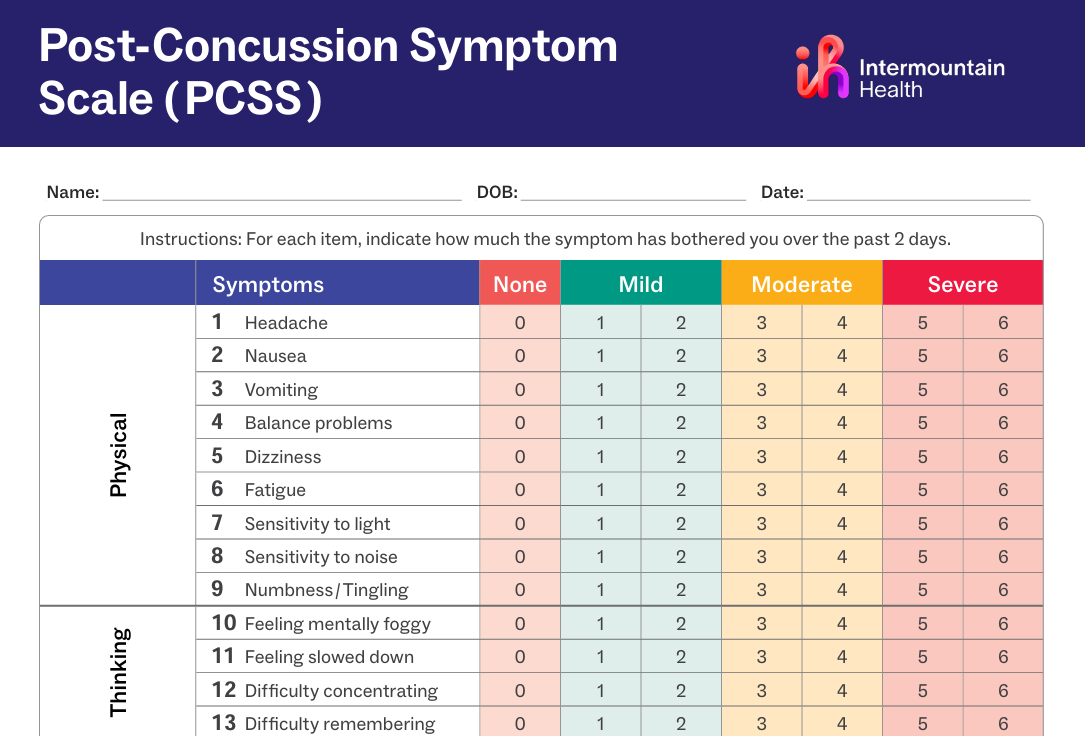
The statistical sensitivity of the PCSS provides definitive thresholds for tracking spontaneous physiological recovery. The total severity index possesses an established Minimal Detectable Change (MDC) of 12.3 points, while the aggregate number of reported symptoms yields a Minimal Clinically Important Difference (MCID) of 5.5 points. Medical providers use these fixed mathematical parameters to validate clinical regression or progress before clearing an athlete to proceed with full return-to-play protocols.
Why Do Rehabilitation Therapists Prefer the Rivermead Questionnaire?
Rehabilitation specialists favor the modified RPQ-3 and RPQ-13 architecture because the scoring matrix actively filters out pre-existing baseline comorbidities. Uniquely, the Rivermead explicitly instructs patients to rate their current symptoms relative to their pre-injury baseline. A rating of 1 indicates the symptom is present but causes no more trouble than usual, and the final scoring algorithm drops it to 0.
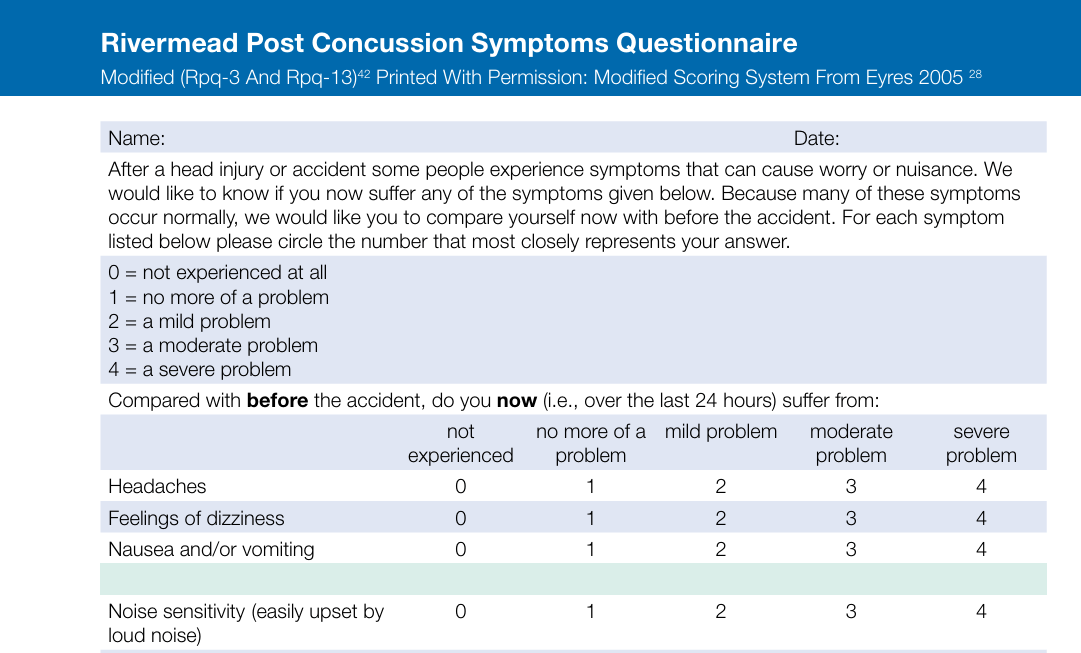
This baseline filtering mechanism prevents pre-existing migraines, learning disabilities, or structural neck pain from artificially inflating the acute injury score. Therapists use this precise baseline separation to identify maladaptive sensory strategies. By isolating the true injury variables, clinicians can implement targeted interventions for individuals who over-rely on visual or surface inputs.

How Do the Subtype Phenotypes Guide Targeted Rehabilitation?
The 16 items on the Rivermead questionnaire divide cleanly into functional clusters, allowing therapists to profile specific concussion phenotypes immediately. Rather than viewing the brain injury as a single systemic problem, therapists split the data to build individualized treatment strategies based on distinct clinical presentations:
Vestibular & Oculomotor Profile (Dizziness, balance problems, blurred vision, double vision): Guides the treatment of sensory mismatch, gaze instability, and poor somatosensory signaling.
Migraine & Somatic Profile (Headaches, light sensitivity, noise sensitivity, nausea): Guides autonomic regulation, dark-room pacing, and progressive habituation.
Cognitive-Fatigue Profile (Forgetfulness, poor concentration, slow thinking, fatigue): Informs cognitive pacing, speech-language therapy, and energy conservation protocols.
The formal separation of the RPQ-3 (headache, dizziness, nausea) from the RPQ-13 (cognitive, emotional, and sleep alterations) alerts the therapist to early physiological deficits versus secondary psychological or cervical overlays. This systemic tracking prevents the development of persistent visual dependency by forcing timely physical integration.
How Can Clinics Bridge the Divide in Outcome Measures?
To optimize clinical efficiency, multi-disciplinary practices should not force therapists or physicians to abandon their preferred metrics.
“Instead, teams must coordinate both instruments across the patient care continuum.”
The PCSS serves as an excellent intake and systemic tracking tool for the physician during medical management. Concurrently, the RPQ provides the precise phenotypic resolution that physical and occupational therapists require to construct highly specific neuromotor retraining exercises. Integrating both tools protects the integrity of the clinical data and accelerates functional recovery timelines.
References
King, N. S., Crawford, S., Wenden, F. J., Moss, N. E. G., & Wade, D. T. (1995). The Rivermead Post Concussion Symptoms Questionnaire: a measure of symptoms commonly experienced after head injury and its reliability. Journal of Neurology, 242(9), 587-592.
Langevin, P., Frémont, P., Fait, P., & Roy, J. S. (2022). Responsiveness of the Post-Concussion Symptom Scale to Monitor Clinical Recovery After Concussion or Mild Traumatic Brain Injury. Orthopaedic Journal of Sports Medicine, 10(10). https://doi.org/10.1177/23259671221127049
Maruta, J., Lumba-Brown, A., & Ghajar, J. (2018). Concussion Subtype Identification With the Rivermead Post-concussion Symptoms Questionnaire. Frontiers in Neurology, 9, 1034. https://doi.org/10.3389/fneur.2018.01034