
Postpartum Vestibular Crisis: Differentiating Superior Semicircular Canal Dehiscence (SSCD) and Perilymphatic Fistula (PLF)

“This clinical briefing for vestibular professionals focuses on the structural divergence between two unique pathological pathways that occur when the high-pressure environment of labor causes a physical breach in the inner ear.
At 10 weeks postpartum, if a patient presents with persistent dizziness and concurrent hearing changes, the clinician must differentiate between failure of the bony labyrinth and failure of the membranous windows.”
Introduction
When a mother is 10 weeks postpartum and still struggling with unsteadiness, the standard clinical narrative often defaults to “postpartum fatigue” or “hormonal shifts.” However, if that patient reports any alteration in her auditory perception, the professional must investigate a mechanical “third window” injury.
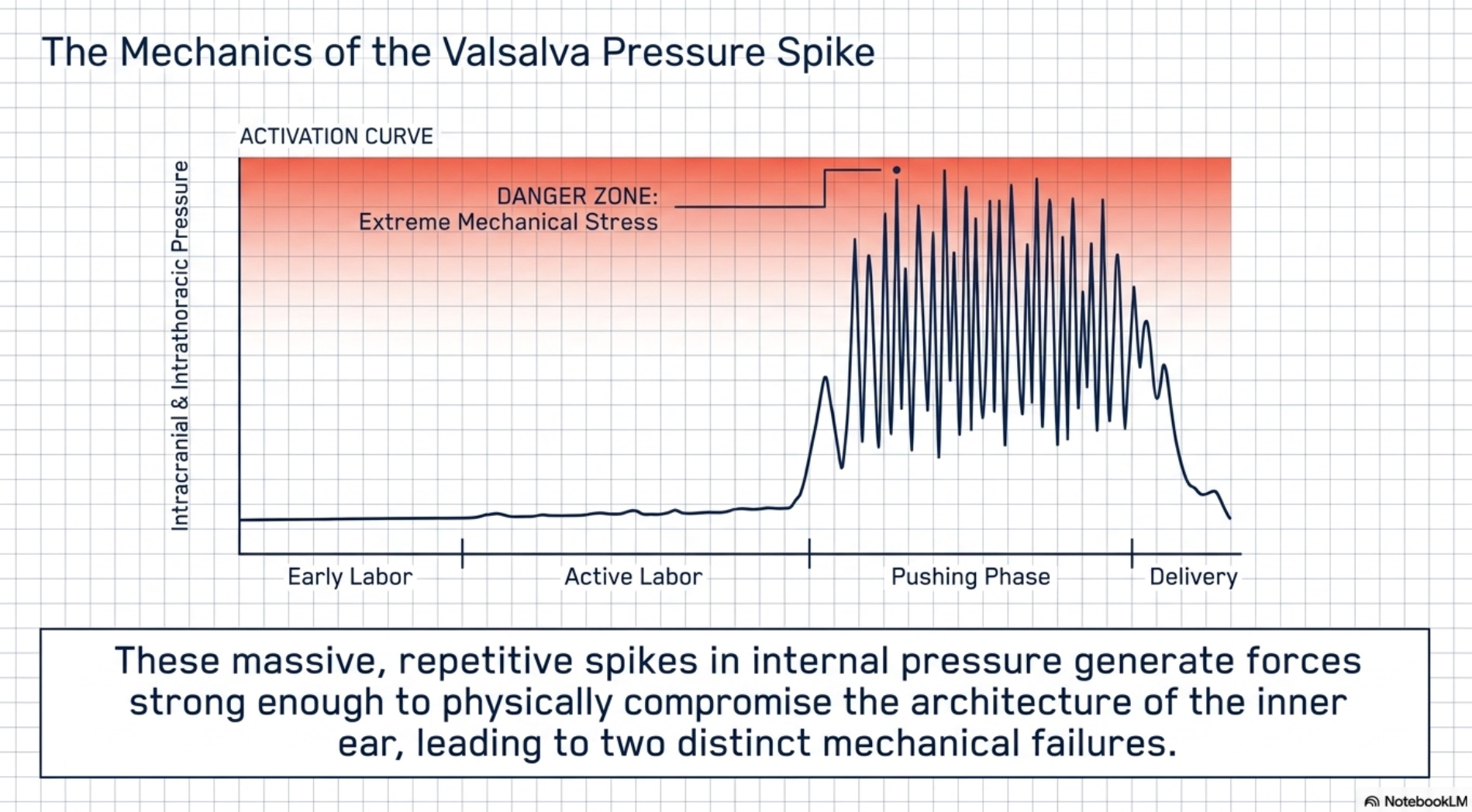
The intense, repetitive Valsalva maneuvers (bearing down) during the second stage of labor create massive spikes in intracranial and intrathoracic pressure that can physically compromise the inner ear hardware.
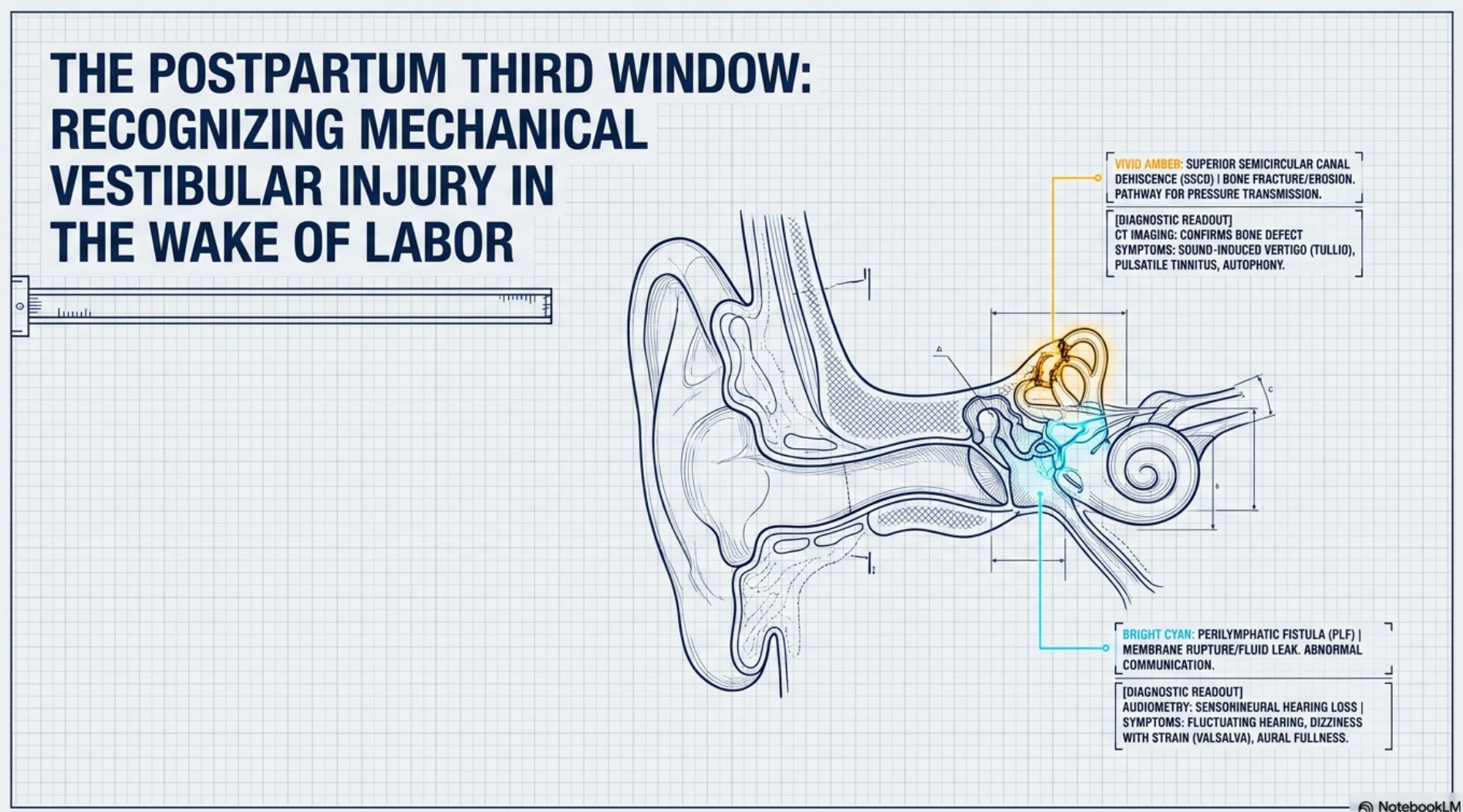
The two primary differential diagnoses in this high-pressure context are Superior Semicircular Canal Dehiscence (SSCD) and Perilymphatic Fistula (PLF). While both result from labor pressure, they represent two distinct pathological pathways involving different anatomical structures and physiological consequences.
Superior Semicircular Canal Dehiscence (SSCD): The Bony Fracture
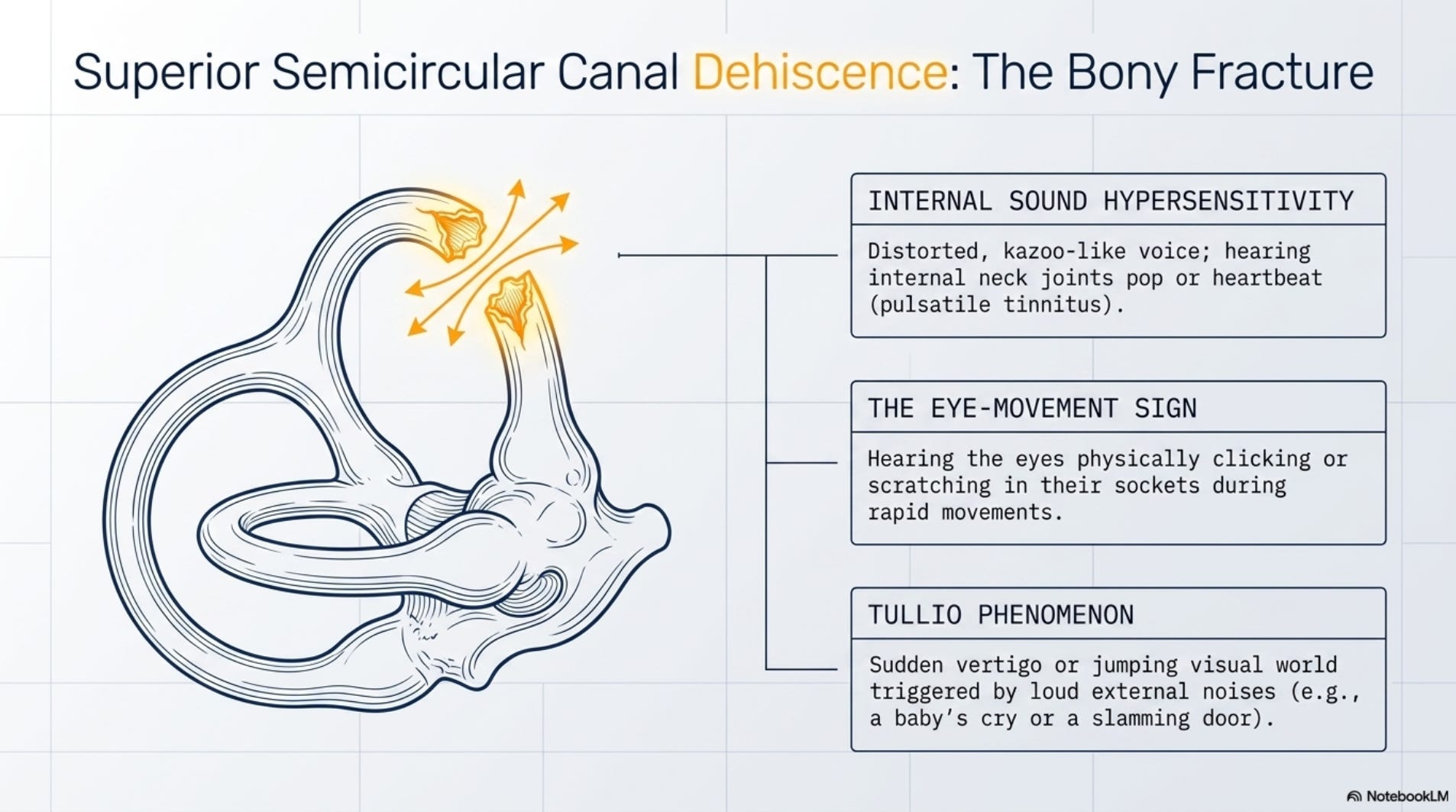
SSCD occurs when the intense intracranial pressure during the pushing phase causes a breach in the thin layer of bone overlying the superior semicircular canal. This creates an abnormal “third window” in the bony labyrinth, allowing sound and pressure to bypass the normal auditory pathway.
Clinical Indicators of Bony Dehiscence:
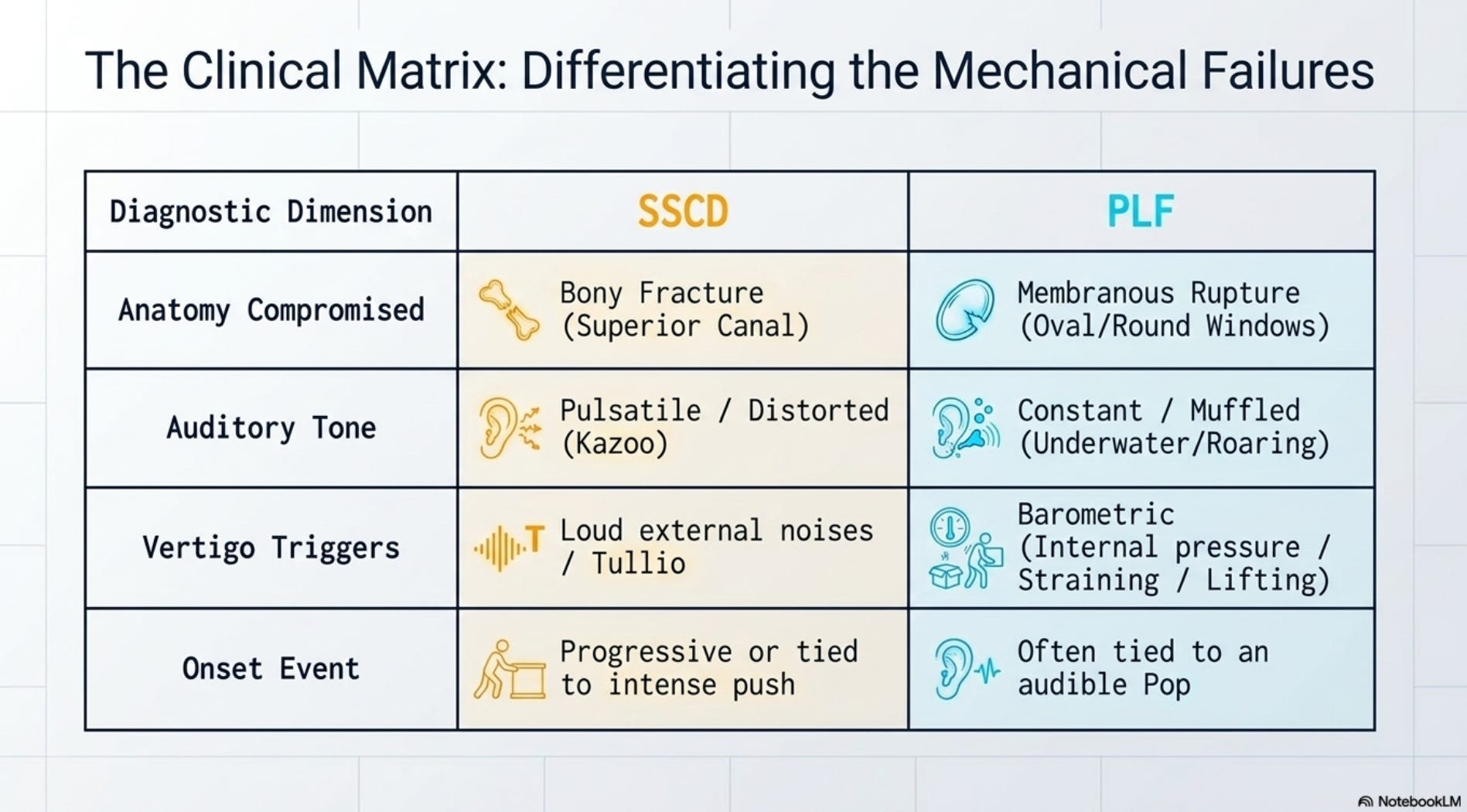
Internal Sound Hypersensitivity (Autophony): The hallmark of SSCD. The patient may report hearing her own voice with a distorted, “kazoo-like” quality, or hearing internal body sounds, such as her heartbeat (pulsatile tinnitus) and popping of her neck joints.
The Eye-Movement Sign: In severe cases, the patient may actually hear her eyes “clicking” or “scratching” in their sockets during rapid eye movements.
Tullio Phenomenon: Vertigo or a sudden “jumping” of the visual world triggered specifically by loud, external noises—such as a baby’s cry or a slamming door.
Perilymphatic Fistula (PLF): The Membranous Blowout
Unlike the bony fracture of SSCD, a perilymphatic fistula is a rupture of the thin membranes of the oval or round windows. This breach allows perilymph (the fluid of the inner ear) to leak into the middle ear space, destabilizing the pressure within the membranous labyrinth.
Clinical Indicators of Membranous Rupture:
Muffled or Fluctuating Hearing: Patients often report an audible “pop” during the most intense phase of labor, followed immediately by a sensation that their hearing is “underwater” or “clogged.”
Pressure-Dependent Vertigo: Dizziness is directly linked to changes in middle-ear pressure. Activities that involve straining—such as lifting the infant, coughing, or blowing the nose—trigger a surge in symptoms.
Roaring Tinnitus: Unlike the pulsatile tinnitus of SSCD, PLF often presents with a constant “roaring,” “hissing,” or “ringing” in the affected ear.
Diagnostic Protocols for the Postpartum “Third Window”
To move beyond a symptomatic description and reach a definitive diagnosis, professionals must employ objective diagnostic testing. When a mother presents with persistent unsteadiness and auditory distortions, the following hierarchy of tests is required to differentiate between Superior Semicircular Canal Dehiscence (SSCD) and Perilymphatic Fistula (PLF).
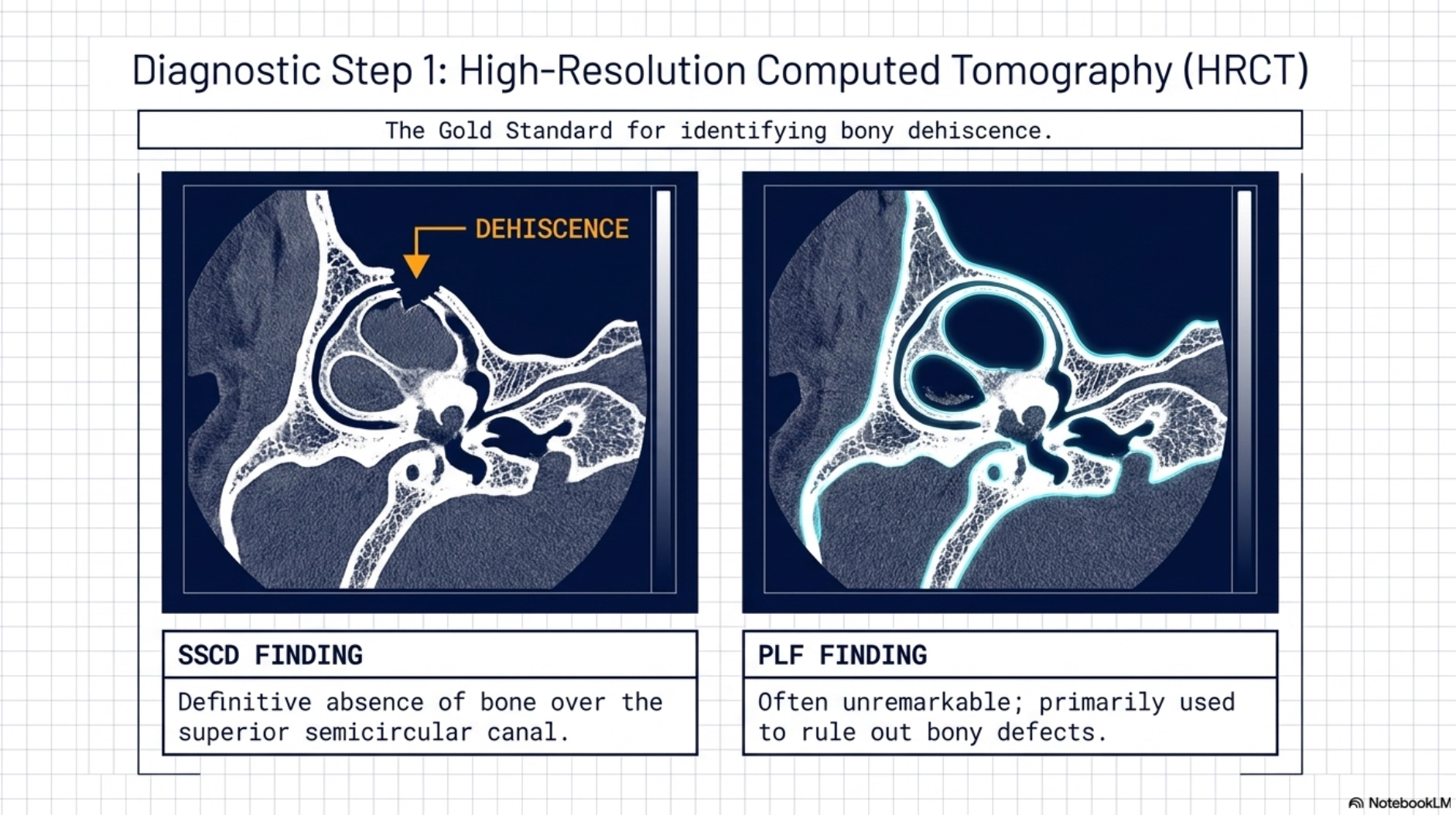
1. High-Resolution Computed Tomography (HRCT)
The gold standard for identifying SSCD is a temporal bone CT scan using specific “sub-millimeter slices” (0.5mm or less).
The Finding: For SSCD, the scan will show a definitive absence of bone (“dehiscence”) over the superior semicircular canal. For PLF, the CT is often unremarkable, making it a primary tool for ruling out bony defects.
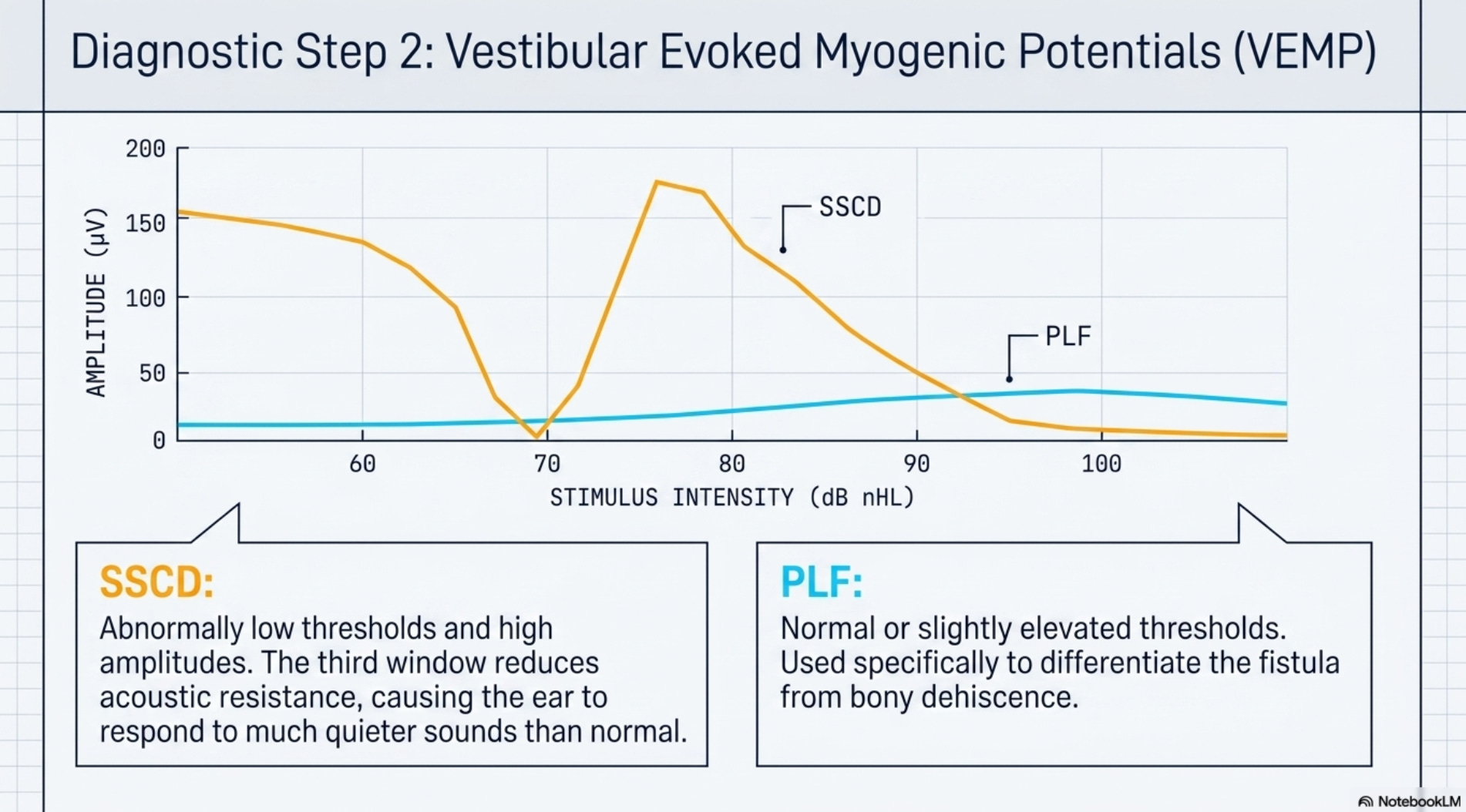
2. Vestibular Evoked Myogenic Potentials (VEMP)
VEMP testing measures the threshold at which the vestibular system responds to sound stimulation.
The Finding in SSCD: Patients demonstrate “abnormally low thresholds” and high amplitudes. Because the “third window” reduces resistance, the ear responds to much quieter sounds than a healthy ear.
The Finding in PLF: Thresholds may be normal or slightly elevated. In PLF, the VEMP is primarily used to differentiate the fistula from a bony dehiscence.
3. Audiometry and Tympanometry
The Finding in SSCD: Testing often reveals an “apparent conductive hearing loss” despite normal middle ear function. This is a “pseudo-conductive” gap because the bone-conduction thresholds are actually better than normal (hypersensitive).
The Finding in PLF: Audiometry typically shows a “sensorineural hearing loss” that may fluctuate. Tympanometry is used to perform a “Fistula Test,” where positive pressure is applied to the ear canal to determine if it triggers nystagmus or vertigo (“Hennebert’s Sign”).
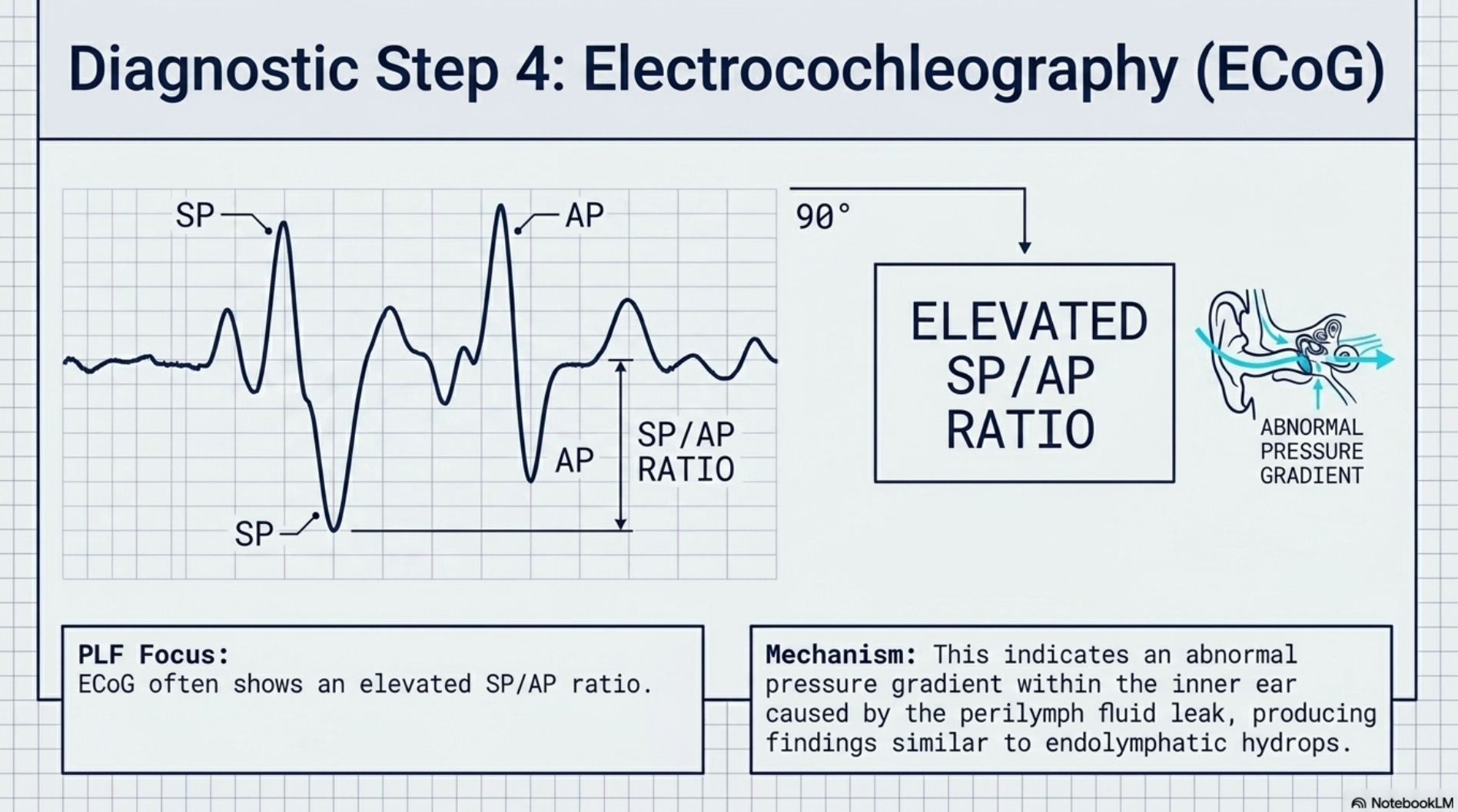
4. Electrocochleography (ECoG)
The Finding: In cases of PLF, the ECoG may show an “elevated SP/AP ratio,” indicating an abnormal pressure gradient within the inner ear due to the fluid leak, similar to findings in endolymphatic hydrops.
Final Professional Summary
At 10 weeks postpartum, the diagnostic focus must shift from general recovery to structural integrity. If the patient hears her heartbeat or eyes, the clinician must investigate a bony fracture (“SSCD”); if she feels “clogged” and recalls a “pop” during labor, the clinician must investigate a membranous blowout (“PLF”). By identifying these structural consequences, the professional moves beyond the “postpartum” label and addresses the actual mechanical failure of the vestibular system.
Clinical Disclaimer: The information provided in this article is for educational and professional development purposes only and does not constitute medical advice. If you are experiencing persistent postpartum dizziness, unsteadiness, or any changes in your hearing, it is imperative that you consult with a medical doctor who specializes in vestibular disorders and advanced diagnostic testing. A thorough evaluation by an Otoneurologist or an ENT specialist with expertise in "third window" pathologies is necessary to determine the underlying cause and ensure appropriate medical or surgical management. Do not attempt to self-diagnose or delay professional consultation, as early identification of structural injuries is critical for long-term recovery.