
PPPD Part 2: Neuroimaging Evidence and the Sensory Role Reversal


Part 1 established the historical transition of Persistent Postural-Perceptual Dizziness (PPPD) into the framework of Functional Neurological Disorders (FND). To understand why patients present with such high levels of body vigilance and avoidance, we must examine the neuroimaging evidence and the specific role reversal of sensory systems. This state is a physiological reality driven by behavioral choices that eventually hard-code a ‘software glitch’ into the nervous system.
Neuroimaging Evidence of Cortical Reorganization
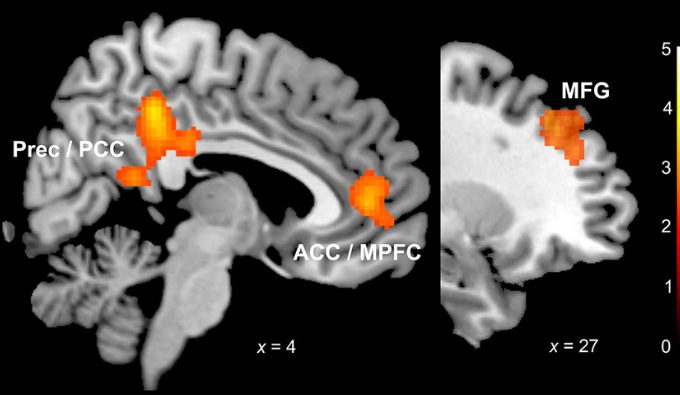
Functional MRI (fMRI) provides evidence that PPPD involves a fundamental shift in how the brain processes spatial information. Research consistently identifies reduced activity and connectivity in the Parieto-Insular Vestibular Cortex (PIVC), the primary hub for vestibular processing.

When a vestibular insult occurs, the brain's higher-level integration centers, including the Anterior Cingulate Cortex (ACC) and the precuneus, often fail to maintain normal communication with the PIVC. The ACC governs threat assessment, while the precuneus handles self-motion perception. In patients with PPPD, these regions show diminished connectivity. This lack of integration leaves the patient in a state of physiological ‘high alert’, where the brain can no longer distinguish between benign environmental motion and actual threats to stability.
Navigators and Stabilizers: The Functional Flip
The core of the PPPD software glitch lies in a maladaptive role reversal of sensory systems. Patients do not just experience a shift in dominance; they fundamentally change how they use their eyes, their bodies, and their inner ears to interact with the world.

The Visual System: From Navigator to Primary Stabilizer
The primary purpose of the visual system is to navigate. It moves us through the environment, allows us to recognize risk, and provides essential depth perception. In a healthy system, the eyes see things coming and allow us to form relationships with the space around us.
In PPPD, the patient makes a behavioral choice to use the visual system as a primary stabilizer. Because they no longer trust their internal balance, they fixate on the visual environment to keep themselves upright. This makes them hypersensitive to any visual movement—busy grocery store aisles or passing traffic—because their stabilizer is now being shaken by the very environment they should be navigating through.

The Somatosensory System: When Stabilizers Begin to Navigate
Typically, the somatosensory system acts as a powerful stabilizer. In PPPD, this system takes on a distorted role. We observe patients seeking out more stable positions, such as sitting, yet they remain profoundly symptomatic. This is because their normal stabilizing system starts to ‘navigate’.
The patient begins to perceive movement through their body that a healthy individual would never recognize. They sense micro-vibrations, subtle sways, or minor shifts in their environment and interpret them as significant motion. They start to ‘feel’ their way through space. This hyper-perception of body-felt movement is a learned, maladaptive strategy. The system designed to keep them steady is now the very system they use to sense a perceived threat of movement.

The Vestibular System: The Distrusted Hardware
As the eyes and body take over, the vestibular system—the actual hardware designed for balance—is compromised in one of two ways:
Hypersensitivity: The brain renders the system hyper-alert to even the smallest head movements, interpreting them as catastrophic.
Inhibition: The brain effectively shuts down vestibular input because it no longer trusts the data, instead relying on visual and somatosensory distortions.
Maladaptive Learning through Behavioral Choice
This sensory role reversal is a direct manifestation of maladaptive learning. When a patient chooses to sit more often to feel ‘safe,’ or chooses to fixate on a horizon line while walking, they are installing a software patch. They believe these modifications are necessary to manage the ‘wacky’ sensations they feel.
Every time a patient chooses these modifications, they reinforce the brain’s reliance on visual and surface dominance. This is not a passive event; it is an active behavioral reinforcement of a flawed premise. Over time, these repeated choices hard-code the glitch, making the software patch feel like permanent hardware. For the vestibular professional, recognizing this flip between navigators and stabilizers explains why the patient perceives almost everything as motion.
Clinical Takeaway
Part 2 reveals that PPPD is a disorder of functional role reversal. The eyes are trying to stabilize what the body should be navigating, and the body is trying to navigate what the ear should be sensing. By identifying these specific shifts, we can see the logic behind the patient’s seemingly irrational behaviors.
Isn't "The patient begins to perceive movement through their body that a healthy individual would never recognize. They sense micro-vibrations, subtle sways, or minor shifts in their environment and interpret them as significant motion. They start to ‘feel’ their way through space. This hyper-perception of body-felt movement is a learned, maladaptive strategy. The system designed to keep them steady is now the very system they use to sense a perceived threat of movement." Same as MdDA?