
Recalibrating Asymmetrical Vestibular Tone in Chronic Unilateral Hypofunction: Advanced Strategies for Spatial Drift


“Asymmetrical vestibular tone refers to a persistent imbalance in the baseline resting firing rates between the left and right vestibular nuclei following a peripheral injury.”
This sensory mismatch disrupts the central nervous system’s internal postural framework, resulting in chronic directional drifting, compensatory nystagmus, and profound exertional fatigue during ambulation. Effective rehabilitation requires targeted neural recalibration and sensory reweighting to resolve this asymmetric tonic drive and restore dynamic postural control.

How Does Asymmetrical Vestibular Tone Simulate a Dual-Engine Aircraft?
To understand the mechanics of chronic vestibular compensation, visualize the bilateral sensory inputs entering the vestibular nuclei as a twin-engine jet aircraft. In a healthy state, both engines produce equal thrust, maintaining a stable, straight-line trajectory. When a peripheral injury occurs, such as a right unilateral vestibular hypofunction, the power output on the right side drops significantly. If the left engine continues to run at 100% capacity while the right engine drops to 70%, the unequal thrust forces the aircraft to yaw.
The question is in which direction.
In the image below, it might turn left toward the more powerful thrust (left-beating nystagmus), but in other situations, it might turn rightward toward the weaker right side (slow phase of nystagmus). This is why tests like the Fuluda March (Utenberget) are inconsistent.
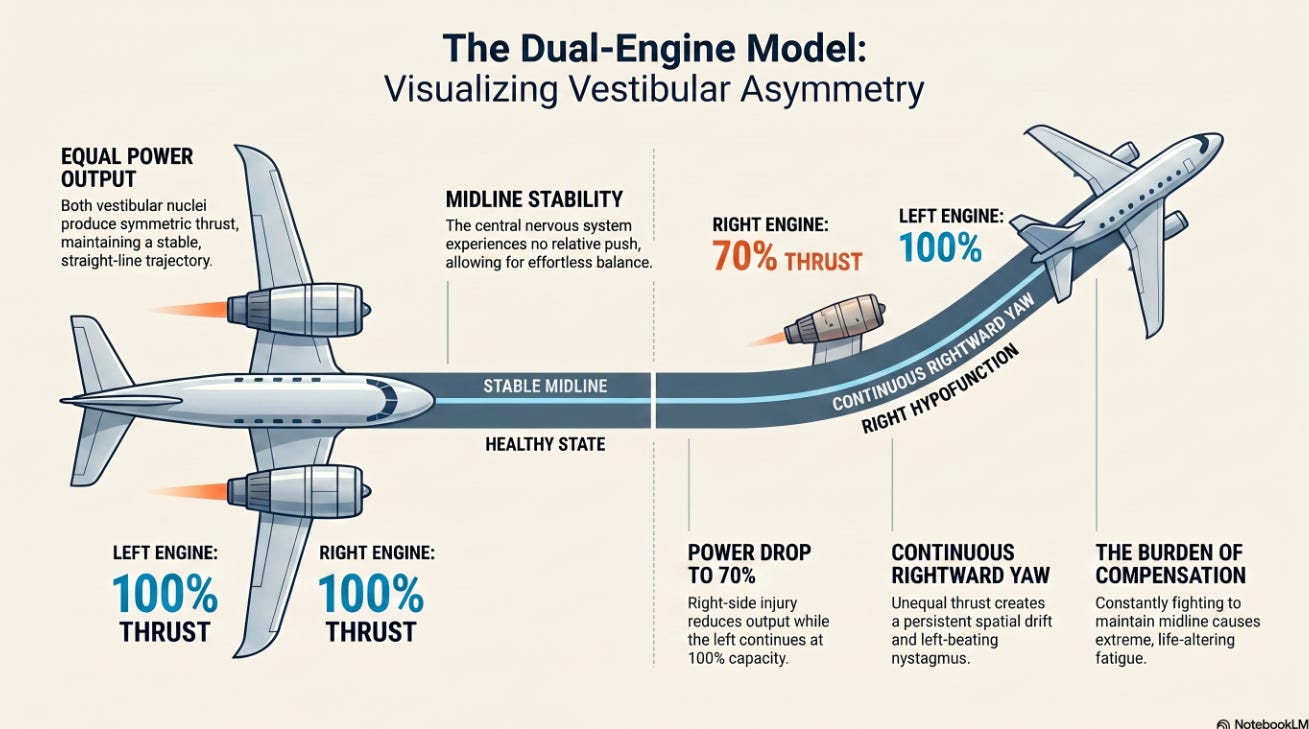
In my opinion, this flight dynamic precisely mirrors the presentation of a patient who suffered a right unilateral vestibular hypofunction 18 months ago. Because the resting discharge rate of the right vestibular nucleus remains lower than that of the left, the central nervous system experiences a relative leftward pull. This asymmetry creates a persistent left-beating nystagmus and induces a constant rightward spatial drift.
The patient must continuously fight to maintain a midline heading. This constant physical and cognitive battle causes extreme fatigue, which frequently incapacitates patients and forces major lifestyle disruptions, such as quitting a retail job to live at a slower, more manageable pace.
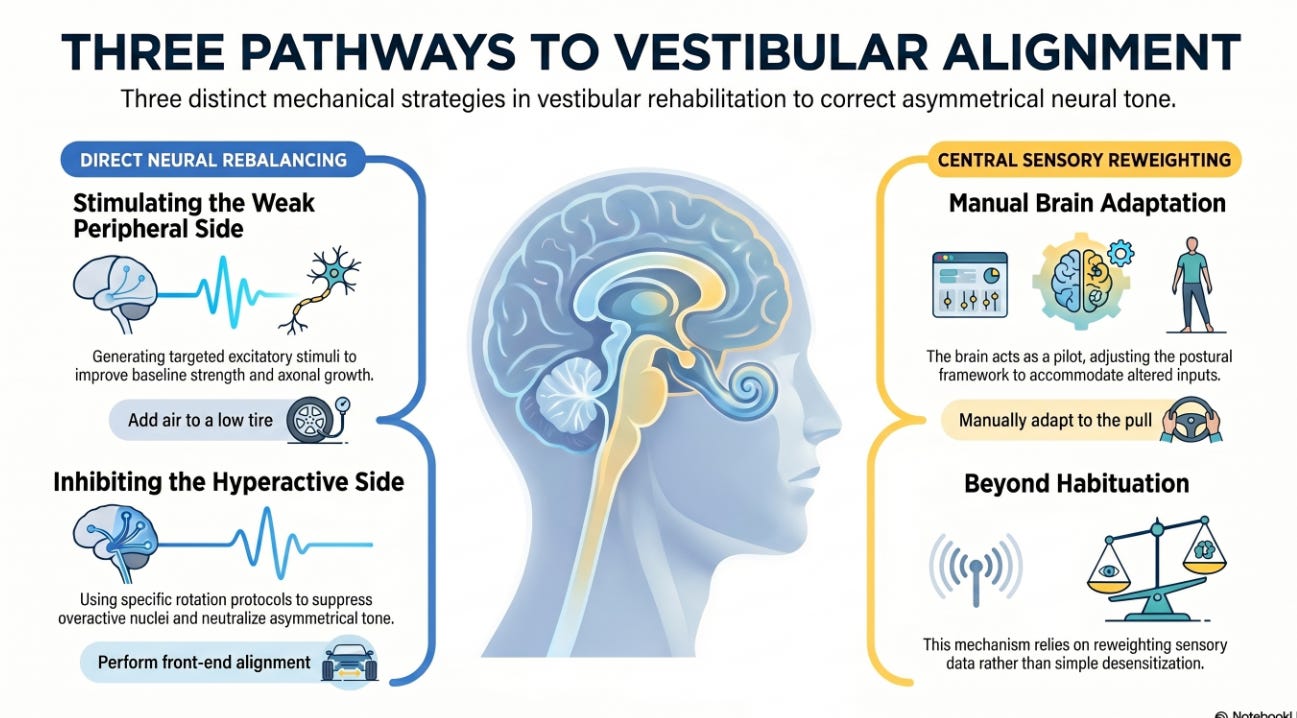
What Are the Primary Mechanical Pathways for Restoring Vestibular Alignment?
When a vehicle’s front end is out of alignment, a driver can manage the pulling steering wheel through three distinct mechanical strategies: add air to a low tire, perform a comprehensive front-end alignment, or manually adapt to the pull through continuous central nervous system compensation.
Vestibular rehabilitation offers parallel pathways to manage asymmetrical tone between the vestibular hemispheres:
Pathway 1: Peripheral Weakness
The first pathway assumes the weak peripheral side retains potential for neural recovery. Rotating the patient to generate a specific, targeted excitatory stimulus to the right lateral vestibular nucleus aims to improve its baseline resting strength and stimulate axonal growth, much like the rehabilitation process for the facial nerve in Bell’s palsy.
Pathway 2: Inhibiting the More Neurally Active Side
The second pathway focuses on inhibiting the opposite, hyperactive side. Clinicians can introduce specific chair-spinning protocols that use alternating short and long spins to suppress the overactive left vestibular nucleus. This post-rotatory stimulus helps neutralize the asymmetrical tone, balancing the baseline inputs between the right and left sides.
Pathway 3: Rebalancing the Front End
The third pathway applies when direct peripheral rebalancing is incomplete. In this scenario, the brain acts as the pilot, manually adjusting the tail rudder and ailerons to keep the aircraft on course. This mechanism does not rely on habituation or desensitization; it uses classic sensory reweighting therapy to adapt the patient’s postural framework to the altered vestibular input.
How Does Asymmetric Proprioceptive Loading Counteract Spatial Drift?
To disrupt a persistent rightward spatial drift, clinicians can introduce an immediate structural counterweight. Placing a 2.5 lb kettlebell exclusively in the patient’s left hand introduces a strong somatosensory component on the side opposite the deviation. This asymmetric load alters the internal center of mass, forcing the central nervous system to dynamically adjust postural tone and correct the rightward trajectory.
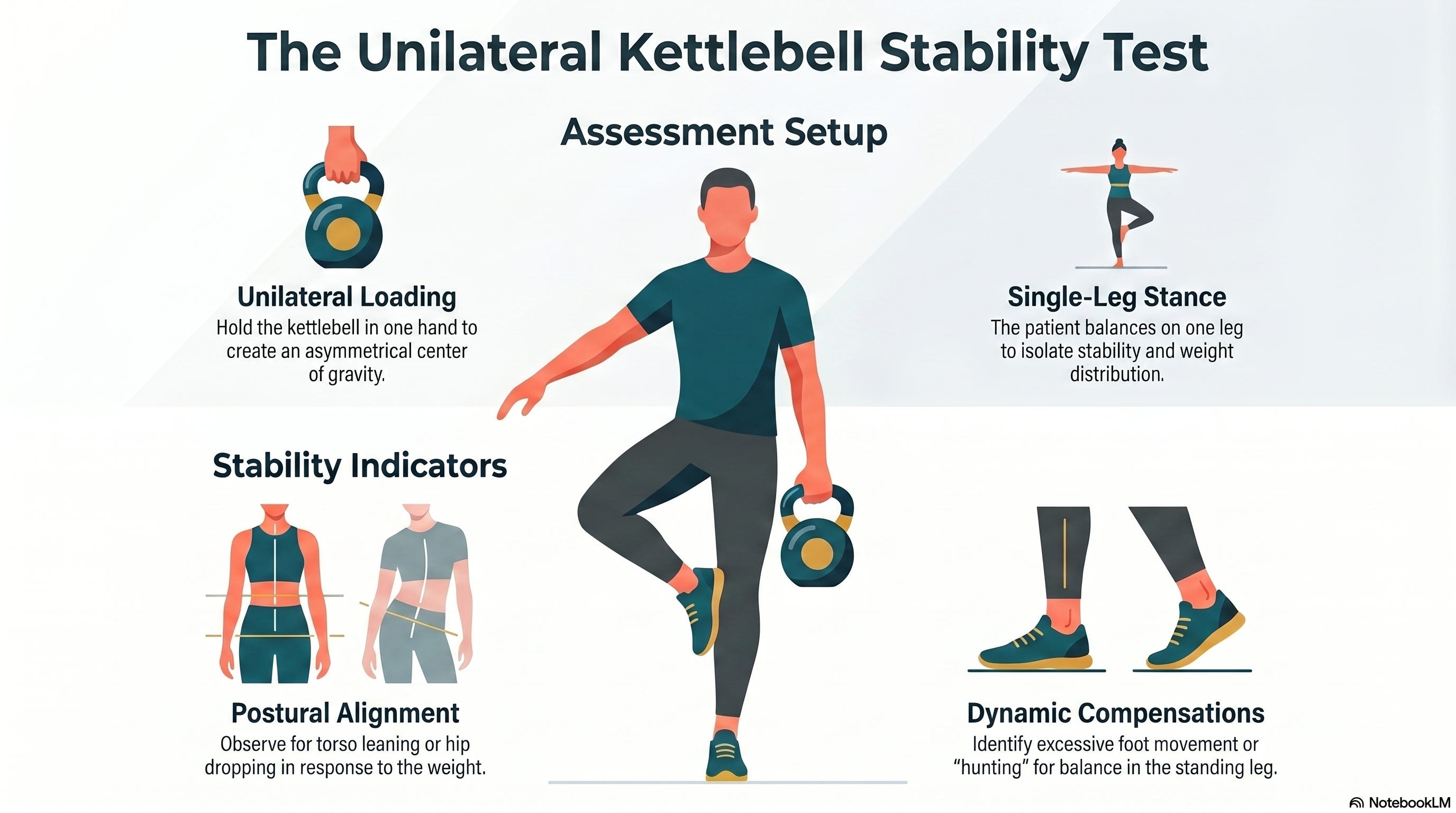
While the patient maintains this left-handed load, the clinician should introduce progressive walking tasks. Instruct the patient to perform forward and backward ambulation across seven distinct head positions. To systematically challenge the central nervous system and prevent reliance on maladaptive patterns, progress these tasks from eyes-open conditions to eyes-closed conditions, and finally into environments that present a high visual conflict.
What Advanced Visual and Roll-Plane Strategies Resolve Recalcitrant Turning Deficits?
Patients with chronic asymmetry often experience severe spatial disorientation during 180-degree turns. Interestingly, a patient may demonstrate an immediate improvement during the second direction or turn they take, regardless of whether they turn right or left. This pattern indicates a neural priming or brief habituation effect, in which the initial rotation exposes a severe sensory mismatch, allowing the central nervous system to organize its motor output more efficiently on the immediately subsequent turn. Clinicians should maintain graded, repetitive turn practice inside a protective corner for safety, systematically increasing rotation speeds, varying the support surface, and requiring strict gaze fixation on a stable target.
To expand the therapeutic toolkit beyond simple gaze stability exercises while walking, clinicians can integrate several collaborative multisensory interventions:
Optokinetic Stimulation: Present optokinetic stripes moving across a screen from right to left while the patient performs reaching or pointing tasks. This specific visual sweep directly counters left-beating nystagmus and helps the brain correct the rightward spatial deviation.
Mirror-Referenced Walking: Place a high-visibility strip of tape down the center of a walkway and position a mirror at the end. This setup forces the patient to rely on a strong visual cue to anchor her trajectory along the midline, actively overriding her distorted vestibular heading.

Roll-Plane Tilt Activities: Evaluate the patient’s Subjective Visual Vertical. If the patient demonstrates a 3-degree rightward Subjective Visual Vertical bias, her brain perceives true vertical as tilted toward the right. Physically tilting the patient 3 degrees to the right aligns the support surface with this distorted estimate of internal vertical. Because her intact visual and somatosensory systems correctly detect that the body is no longer truly upright, this alignment creates a deliberate multisensory conflict, forcing the central nervous system to reweight its available inputs and gradually correct the perceptual error back toward true vertical.
Why Is a Comprehensive Biomechanical Screening Essential for Vestibular Compensation?
Effective vestibular adaptation requires a structurally sound musculoskeletal framework. Clinicians must conduct a comprehensive biomechanical screening to rule out peripheral or structural contributors to gait deviation and lateral drift:
Distal Sensation: Screen for subtle sensory or proprioceptive deficits at the feet and ankles that might impair accurate ground-reaction feedback.
Quadriceps Lag: Evaluate the patient for quadriceps lag, which results in an unstable, slightly bent knee during the weight-bearing phases of gait, thereby destabilizing forward progression.
Hip Abductor Strength: Assess for gluteus medius weakness that results in a Trendelenburg gait, directly impairing lateral pelvic stability and forcing lateral compensation.
Visual Fields and Gaze Focus: Track exactly where the patient directs her eyes during ambulation. If the patient habitually looks toward the right side of her environment, her body will naturally follow her gaze, compounding her baseline vestibular spatial drift.
Conclusion: Driving Recalibration Through Precision Sensory Reweighting
Resolving a persistent spatial drift and asymmetrical tone 18 months after a unilateral vestibular injury requires moving away from repetitive, non-specific habituation protocols. When a chronic right unilateral vestibular hypofunction leaves the central nervous system trapped in a maladaptive sensory strategy, clinicians must deploy precise, structured interventions to restore equilibrium. Whether maximizing remaining peripheral output through targeted acceleration, neutralizing asymmetric tone via short and long chair-spinning protocols, or modifying the internal center of mass using asymmetric proprioceptive loading, the objective remains clear: force the brain to abandon its distorted internal baseline and actively reweight its available sensory streams.
“Integrating strategic multisensory inputs—such as optokinetic stimulation, mirror-referenced walking, and roll-plane tilt adjustments—provides the central nervous system with the clear, unambiguous visual and somatosensory anchors it needs to correct spatial errors and reconstruct an accurate estimate of verticality.”
When these advanced vestibular techniques are paired with a comprehensive biomechanical screening to eliminate peripheral tracking errors, clinicians can systematically dismantle chronic compensation barriers. This integrated framework transitions the patient away from exhausting, conscious compensation and guides them toward true, automated neural recalibration, ultimately restoring both postural stability and functional independence.
Thanks for clearly explaining a complex yet important health aspect.