
Redefining Recovery: Why Normal Function is the Clinical Standard in PPPD


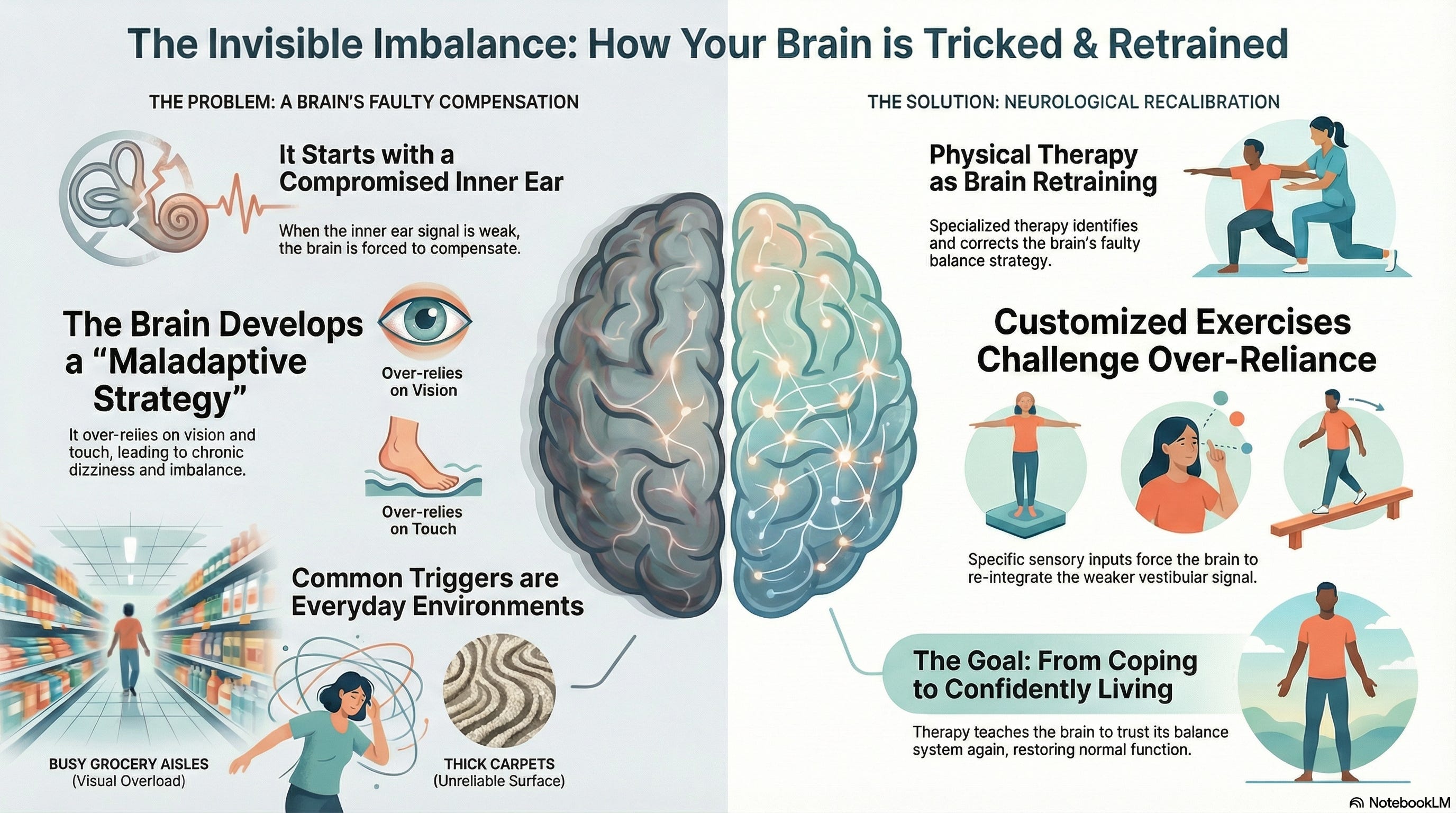
A colleague recently raised an important question regarding my infographic, ‘The Invisible Imbalance’. The graphic concludes with the goal of ‘restoring normal function,’ yet I often state that we do not necessarily ‘cure’ Persistent Postural-Perceptual Dizziness (PPPD) in the traditional sense. This distinction is not merely semantic; it is a clinical reality that dictates how we manage expectations and design treatment protocols for the chronic vestibular patient.
The Trajectory of Functional Imbalance
As the infographic illustrates, PPPD typically starts with a ‘compromised vestibular system’. This initial insult can take many forms, including peripheral vestibular injuries or central events like a ‘stroke or injury to the balance center’ in the brain. Whether the trigger is a viral infection of the nerve or a vascular event in the brainstem, this ‘hardware’ compromise forces the brain into an emergency processing state.
While the physical damage may stabilize, the primary pathology in PPPD is the brain’s failure to return to baseline once the threat has passed. Instead, the brain develops a ‘maladaptive strategy’ of compensation. It adopts a high-gain monitoring state, becoming hyper-vigilant to motion and visual stimuli while disregarding reliable balance data.
Defining Normal Function through Recalibration
When a patient or professional seeks a ‘cure,’ they are often looking for the total erasure of this neurological blueprint. However, since the issue is a software recalibration rather than a physical lesion, our clinical objective is not to ‘delete’ the past, but to overwrite it with more efficient processing.
‘Normal function’ is defined by the restoration of ‘functional independence’ and the elimination of the handicap associated with the condition. It means the brain has achieved a state of ‘neurological recalibration’.
Beyond Passive Habituation: We must move away from the perception of habituation—merely ‘getting used to’ an error—and toward active recalibration.
Adaptation Training: Unlike habituation, which seeks a non-response, adaptation is a proactive recalibration. We are not just training the brain to ignore the noise; we are training it to ‘respond differently’ to sensory input.
Sensory Re-weighting: Through ‘customized exercises’, we provide specific sensory inputs to force the brain to ‘re-integrate the weaker vestibular signal’. We recalibrate the sensory hierarchy so the brain once again prioritizes vestibular data over ‘visual overload’ or over-reliance on touch.
From Coping to Confidently Living
The goal for our patients is to move from ‘coping’—where they are managing symptoms—to ‘confidently living’—where they are no longer aware of their balance system.
We achieve ‘normal function’ when the brain stops over-monitoring balance, and the patient can navigate ‘busy grocery aisles’ or walk on ‘thick carpets’ without the need for conscious guarding or postural bracing. Success is not measured by the total absence of any future dizzy sensation, but by the fact that those sensations no longer control the patient’s life. We are not fixing a broken part; we are training a resilient system.
Clinical Takeaways for the Vestibular Professional
Validate the Initial Injury: Recognize that PPPD typically starts with a ‘compromised vestibular system’—whether via peripheral injury or a central event like a ‘stroke’—but treat the resulting ‘maladaptive strategy’.
Prioritize Recalibration: Focus on active ‘adaptation’ and ‘sensory re-weighting’ to fix the processing error rather than settling for passive desensitization.
Define Success by Autonomy: Educate patients that a lack of a ‘cure’ for their underlying sensitivity does not prevent a return to ‘normal function’ and a life lived with confidence.
Solid distinction between fixing hardware vs recalibrating software in the brain. The comparison to overwriting a neurological blueprint instead of deleting it makes way more sense than just habituation alone. I've seen patients get stuck in that coping phase, constantly guarding movements, when the real shift happens once they retrain sensory hirearchy and stop over-monitoring every step.