


When a patient presents with a classic history of positional vertigo but shows completely negative findings on the standard bilateral Dix-Hallpike test, the case warrants a closer look at the vestibular system's fluid dynamics. This specific presentation highlights a 45-year-old female with idiopathic positional symptoms who consistently noted that her vertigo felt significantly worse when sitting up rather than when lying down in bed.
Why the Standard Dix-Hallpike Descent Produces Zero Nystagmus
When a patient presents with short-arm benign paroxysmal positional vertigo, the initial descent into the Dix-Hallpike position does not provoke the classic paroxysmal nystagmus. This silent descent often leads clinicians to rule out posterior canal involvement entirely.
The biomechanical explanation lies in the exact resting position of the free-floating otoconia. Because the debris is trapped inside the short arm of the posterior semicircular canal—located between the utricle and the cupula—the physical movement of dropping backward into the diagnostic position fails to create a significant linear displacement of the particles away from or toward the cupula. Without particle movement, the endolymph remains static, the cupula remains undeflected, and zero nystagmus or subjective vertigo occurs on the descent.
What Happens When the Patient Sits Up?
A critical mechanical transition occurred when moving the patient from the right Dix-Hallpike position back up into a long sitting position. Once she reached the top of the seated position, an intense, immediate upbeat torsional nystagmus developed.
The nystagmus displayed specific diagnostic characteristics:
It was highly enhanced under infrared video goggles compared to fixation in the light.
It demonstrated a prolonged, lingering duration that lasted between 2 to 3 minutes before finally resolving.
The response was fully repeatable upon subsequent trials.
When the patient sits up from the right Dix-Hallpike position, gravity forces the free-floating debris within the short arm to move utriculofugally (away from the utricle). In the vertical posterior semicircular canal, a utriculofugal movement of endolymph pulls the cupula away from the vestibule, which creates an excitatory stimulus. This intense excitation directly drives the robust upbeat torsional nystagmus observed under the goggles. Because the debris settles heavily against the cupula in this upright alignment, the stimulus lingers, remaining prolonged and non-fatiguing until the neural response slowly habituates or desensitizes over a 2- to 3-minute window.
The Biomechanics of the Inversion Test and Reversing Nystagmus
To expose short-arm pathology, clinicians must manipulate gravity to move particles. When you transition the patient into the nose-down inversion test, gravity pulls the free-floating otoconia from the short arm back toward the utricle.
This mechanical shift creates an ampullopetal fluid flow, pushing the endolymph toward the ampulla. In the posterior canal framework, ampullopetal movement delivers an inhibitory stimulus. Instead of seeing the classic excitatory upbeat torsion, this inhibitory shift suppresses the right posterior canal’s resting discharge, which unmasks a clear reversal of the nystagmus direction.

Why Inhibiting the Right Posterior Canal Provokes a Left Downbeat Torsional Response
The appearance of a downbeat torsional nystagmus beating toward the left during a right-sided short arm inhibition often causes diagnostic confusion.
To interpret this pattern correctly, clinicians must analyze the shared geometric planes of the vestibular system.
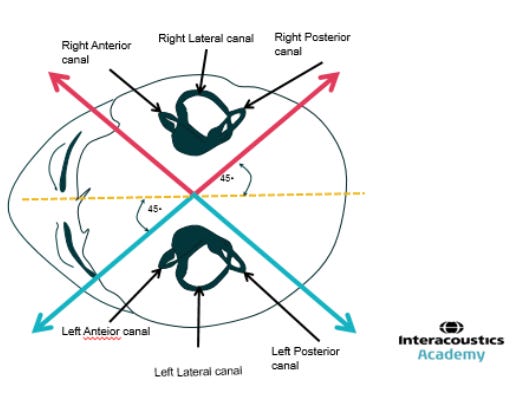
The semicircular canals function in pairs across the head. The right posterior canal is aligned in the exact parallel plane as the left anterior canal. Because of this paired structural organization, suppressing the neural output of the right posterior canal disrupts the balanced baseline signaling between the two ears.
When the resting discharge of the right posterior canal drops due to ampullopetal inhibitory debris movement, the central nervous system interprets this relative difference as a net excitation of its paired partner, the left anterior canal. Activating the left anterior canal pathways reflexively drives the extraocular muscles to produce a downbeat torsional nystagmus beating directly toward the left side.
The Short Arm Treatment Protocol
Managing short arm canalithiasis requires a deliberate departure from standard repositioning procedures. Identifying the presentation as a case of sitting up vertigo is the vital first step. Once confirmed, the treatment logic focuses on using gravity and mechanical agitation to guide the trapped otoconia out of the short arm and back into the utricle.

The execution of this specialized protocol follows a strict sequence:
Immediate Nose-Down Positioning: Hold for 3 minutes.
Place the patient into an immediate nose-down position on the opposite side of the affected canal. For this right posterior canal presentation, the patient is positioned nose-down on the left side.
This position mirrors the final nose-down stage of a standard Epley maneuver or a Semont variation, maximizing the gravitational draw on the short arm back toward the utricular opening.
Mechanical Agitation (Head Shaking): 10 to 15 seconds every 30 seconds.
While maintaining the nose-down alignment, introduce mild head shaking for 10 to 15 seconds. Repeat this oscillation every 30 seconds throughout the 3-minute hold. This targeted agitation helps dislodge the free-floating otoconia from the tight anatomical confines of the short arm, preventing them from adhering to the cupula or remaining trapped by local fluid resistance.
Patient Re-Erection and Rest: Hold for 5 minutes.
Slowly return the patient to an upright seated position. Allow the patient to rest quietly for 5 minutes to allow the endolymph to stabilize and ensure that the otoconia settle completely within the utricular matrix.
Following the application of this protocol, a comprehensive reassessment was performed. Upon moving from the lying-down position back to sitting up, the patient demonstrated complete resolution of both upbeat torsional nystagmus and subjective sitting-up vertigo, confirming the clinical efficacy of the maneuver.