
The Activity Paradox: When High Function Masks A Complex Vestibular Dysfunction


As vestibular specialists, we frequently encounter the ‘high-achiever‘—the patient who refuses to let dizziness dictate their life. They are driving, working out, and managing complex households. On paper, their ‘activity levels‘ suggest they should be well into the habituation phase of recovery. However, their clinical presentation tells a different story: chronic ‘heaviness‘, ‘facial pressure‘, ‘eye strain‘, and a persistent baseline of ‘sensory mismatch‘.
1. Beyond VVM: Understanding the VSVM Strategy
In 1996, Art Mallinson and Neil Longridge identified the ‘Visual Vestibular Mismatch‘ (VVM), describing patients who become highly ‘visually dependent‘ following a vestibular insult. These patients ‘anchor‘ their world through their eyes because the vestibular ‘signaling‘ is unreliable.
However, we often see a more complex and debilitating evolution: the VSVM (Vision > Somatosensory > Vestibular) pattern. In a VSVM strategy, the patient is not only ‘visually dependent‘ but also ‘surface-dependent ‘. This dual dependency is typically the hallmark of a patient with profound vestibular hypofunction or a highly complex, uncompensated disorder.
The paradox is that while a ‘VSVM‘ strategy usually leaves a patient bedridden, the ‘high-achiever‘ is forcing this ‘bedridden software‘ to run at 70 mph. They are ‘moving‘, but they are not ‘adapting‘.

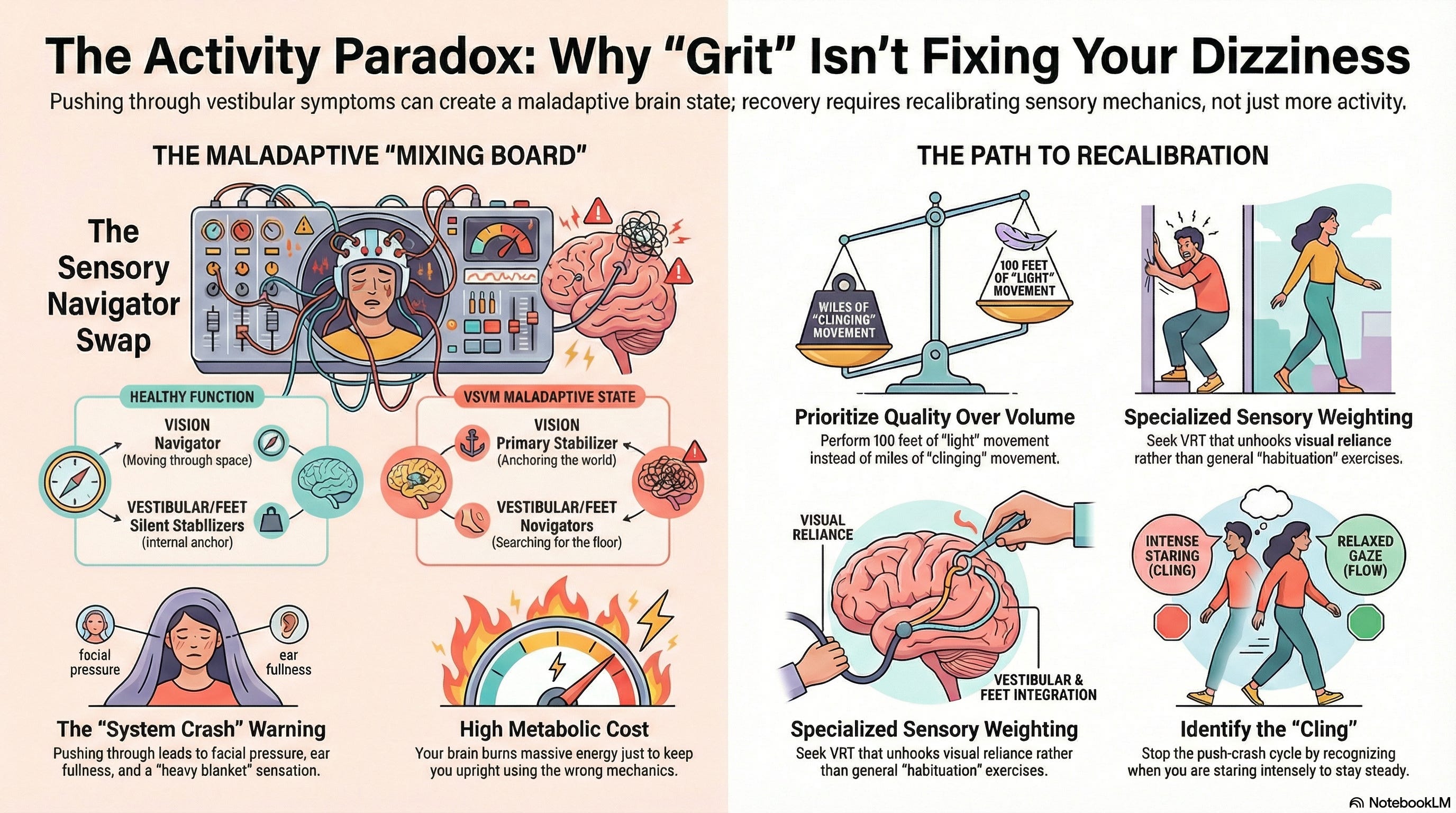
2. The Mechanics: Navigators vs. Silent Stabilizers
To ‘recalibrate‘ these patients, we must understand the ‘pathological swap‘ occurring on their internal ‘mixing board‘. Each sensory system has a primary and secondary role in the hierarchy of balance that has been functionally reversed:
Vision: Primarily a Navigator. In VSVM, the brain pushes this ‘fader‘ to the top, thereby making vision the primary Stabilizer. The eyes are now trying to ‘anchor‘ the environment rather than ‘navigating‘ it. This leads to ‘awful pain behind the eyes‘ and ‘visual irritability‘.
Vestibular System: Primarily a Silent Stabilizer. In these patients, the ‘integrity‘ of the signal is so low—or the ‘signaling‘ is so noisy—that the brain has functionally ‘faded it out‘ to avoid conflict.
Somatosensory System: Primarily a Silent Stabilizer. In VSVM, the brain uses the ‘surface‘ (feet and joints) as a Navigator. The patient ‘searches‘ for the floor, leading to the sensation of walking through a ‘soaked blanket‘ or feeling ‘super heavy‘.
3. The High Metabolic Cost of Compensation
Think of this patient like a golfer who is overswinging or a pitcher with broken mechanics. They can ‘throw the ball‘ with 100% effort, but if their technique is fundamentally flawed, ‘throwing harder‘ only reinforces the error.
In vestibular terms, ‘doing more‘ with a maladaptive sensory strategy only deepens the neurological groove of the mismatch. Because they are using their eyes and feet to do the job of their ears, any complex ‘microenvironment‘—a crowded store, a busy gym, or an uneven trail—triggers a ‘system crash‘.
The resulting ‘facial pressure‘, ‘ear fullness‘, and ‘sound sensitivity‘ are the ‘exhaust fumes‘ of a system running at an unsustainable ‘metabolic cost‘. They aren’t ‘recovering‘; they are ‘compensating‘ at a rate that leads to total systemic exhaustion.
4. Clinical Path: Recalibration (Adaptation) Over Habituation
For this patient demographic, ‘generalist‘ VRT—focused on simple habituation or basic balance drills—is insufficient. You cannot ‘habituate‘ a VSVM strategy. You must recalibrate it.
The professional must:
Facilitate an environment that ‘unhooks‘ the visual ‘anchor‘, forcing the brain to stop over-stabilizing with the eyes.
Support the Somatosensory system so it returns to its role as a Silent Stabilizer, lifting the ‘heaviness‘ the patient feels.
Optimize the Vestibular ‘integrity‘ and ‘signaling‘ so the brain eventually trusts its primary anchor again.
Coordinate the Strategy: We must teach the patient that ‘grit‘ is not the solution for a ‘neurological glitch‘. Success requires shifting focus from ‘volume of activity‘ to ‘integrity of strategy‘.
Clinical Assessment: Identifying the Active VSVM Patient
When evaluating a high-functioning patient, look for these specific ‘signs‘ that indicate a ‘VSVM‘ strategy is masking their progress:
Objective SOT Data: Look for ‘Visual Dependency‘ (low Ratios 2, 3, 5, 6) combined with ‘Surface Dependency‘ (low Ratio 4).
The Lead Blanket Complaint: Patients describe their bodies as ‘heavy‘ or ‘guarded‘ despite having 5/5 manual muscle strength.
Visual-Facial Pressure: Complaints of ‘sinus-like‘ pressure or ‘ears that won’t pop‘ that spike specifically during visual navigation tasks.
Mechanical Over-Drive: The patient is doing ‘more‘ but feeling ‘worse‘, indicating they are reinforcing a ‘maladaptive strategy‘ through high-volume repetition.
Thanks for this...does explain a lot...I continue with the circular dots for MdDS and go on with work and living.
I hadn’t thought about it but bet this explains my perceived quads weakness when getting up from sitting. Since I got a free gym membership with my Medicare Advantage I started doing leg days twice a week there and really don’t have any weakness compared to a few decades ago. But I am working up anyways as I enjoy it.