

The Casani Maneuver: Precision Treatment for Short-Arm Horizontal Canal BPPV - Apogeotropic - Part 1


The Casani maneuver, a technique that is gaining momentum in modern vestibular rehabilitation, has its roots in the pioneering work of Dr. Augusto Pietro Casani. While the specific publications detailing his initial findings may be limited, his clinical observations and techniques have been passed down and refined. Dr. Casani's contribution focused on developing a liberation maneuver tailored to the unique challenges of horizontal canal BPPV, mainly when otoconia are adherent to the cupula. His work, which emphasized the importance of rapid head movements to dislodge debris, laid the groundwork for the push-pull dynamics we explore today. It is important to note that the maneuver is often compared to the Semont maneuver, which was initially published in 1988 by Semont and Sterkers.
Expansive Context: Dr. Casani's work is significant as it provides a targeted approach for a specific and often challenging presentation of BPPV. Due to its anatomical orientation, the horizontal canal presents unique challenges in diagnosis and treatment. His work recognized that standard posterior canal maneuvers were often ineffective for horizontal canal BPPV, prompting the development of a specialized technique. By focusing on rapid head movements, Dr. Casani's method aimed to create sufficient inertial forces to dislodge adherent otoconia, a critical consideration when dealing with cupulolithiasis or tightly packed canalithiasis within the horizontal canal.

Imagine this: A patient walks into your clinic complaining of severe vertigo. You begin your assessment, suspecting horizontal canal BPPV. You meticulously identify the affected side and determine that the debris is likely attached to the cupula, but you are unsure whether it's on the short or long arm. However, you do know that recent research suggests that many horizontal apogeotropic canal disorders are due to short-arm involvement. The persistent nystagmus indicates that the otoconia are stubbornly clinging to the cupula. Traditional repositioning maneuvers aren't cutting it. What's your next move?
This is where the often underused Casani maneuver can be a game-changer. With its unique approach and seemingly counterintuitive movements, the Casani can feel perplexing. However, fear not, fellow vestibular therapists! This article, Part 1 of a two-part series, will demystify the Casani maneuver, focusing specifically on likely short-arm debris. Armed with this knowledge, you will be equipped to tackle these persistent horizontal canal BPPV cases, potentially transforming patient outcomes and instilling hope in you and your patients.
Clinical Observation: Prevalence of Likely Short-Arm Debris
Recent literature and clinical observations suggest that otoconia in horizontal canal BPPV, particularly the apogeotropic variant, are frequently associated with the cupula's short arm (utricular side). This is often attributed to the patient's sleeping habits. Many individuals with horizontal canal BPPV tend to sleep on the affected ear side, which allows debris to accumulate on the short arm of the cupula due to gravitational forces. This underscores the clinical relevance of understanding and effectively treating likely short-arm horizontal canal BPPV.
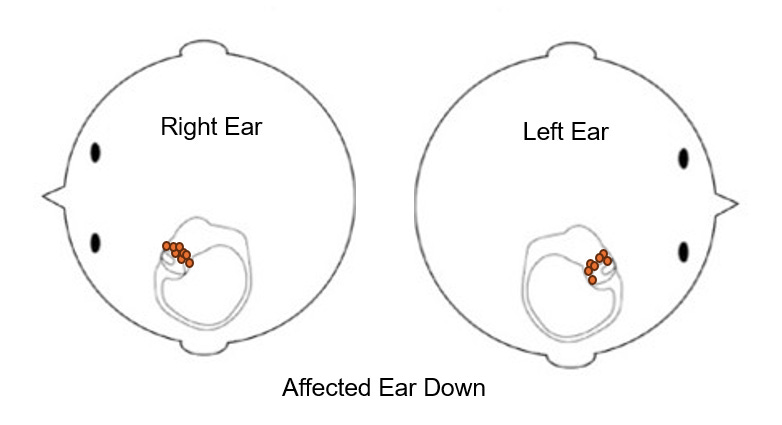
Expansive Context: The prevalence of likely short arm debris in apogeotropic horizontal canal BPPV is a significant clinical consideration. This is because it directly influences the choice of treatment strategy. By understanding the common etiology of this presentation, clinicians can better anticipate the probability of debris location and implement appropriate maneuvers. Furthermore, this observation emphasizes the importance of patient education regarding sleep hygiene during and after BPPV treatment, making us feel responsible and proactive in our approach.
Liberating Otoconia: The Casani's Purpose (Likely Short-Arm Debris)
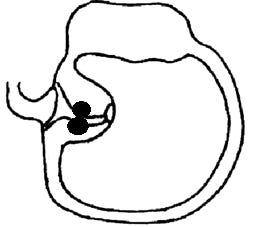
The Casani maneuver aims to liberate the otoconia that are likely adhered to the short arm of the cupula within the horizontal canal. This liberation is achieved through a two-step process:
Rapid Head Movement: The patient is quickly laid down on one side, creating a sudden shift in head position. This rapid movement helps to dislodge the otoconia from their likely attachment to the cupula.
Secondary Head Movement (Gufoni Position): The head is turned 45 degrees down. This specific head position, known as the 'Gufoni head position,' further guides the otoconia away from the cupula and toward the utricle, where they can no longer cause vertigo.
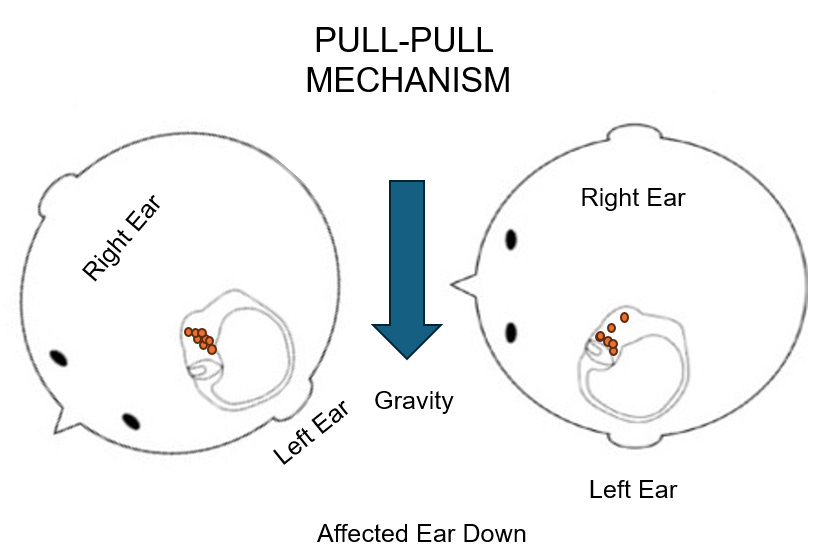
Push vs. Pull: The Core Mechanism (Likely Short-Arm Debris)
The Casani maneuver uses the principles of 'push' and 'pull' to liberate otoconia from the likely short arm of the cupula.
Push: The goal is to push the otoconia off the cupula. This is achieved by rapidly moving the patient to the unaffected ear side, followed by the Gufoni head position. This move places the patient in an excitatory position.
Pull: The goal is to pull the cupula away from the otoconia. This is achieved by rapidly moving the patient to the affected ear side, followed by the Gufoni head position. This is an inhibitory position.
The Excitatory and Inhibitory Considerations (Likely Short-Arm Debris)
Push (Unaffected Ear): Moving the patient to the unaffected ear side for a push effect places them in an excitatory position. This could elicit a more intense vertigo response.

Pull (Affected Ear): Moving the patient to the affected ear side for a pull effect places them in an inhibitory position. This may be a gentler approach, potentially reducing the intensity of vertigo.
The Push and Pull Dynamics: A Closer Look (Likely Short-Arm Debris)
The terms 'push' and 'pull' might seem abstract when discussing the Casani maneuver. Let's break down what these mean in terms of the otoconia and the cupula:
Push: When discussing a 'push' effect, we try to push the otoconia off the cupula and guide them out of the short arm directly into the utricle. This is achieved by rapid head movement towards the unaffected side, followed by the Gufoni head position (45 degrees nose down). Think of it like driving a car fast with food in the middle console. You push the debris, and then you hit the brakes! The debris keeps going!
Pull: In contrast, a 'pull' effect involves pulling the cupula away from the otoconia. This is achieved by the rapid head movement towards the affected side, followed by the Gufoni head position. Imagine holding a tablecloth with crumbs and pulling it away quickly – the crumbs (otoconia) stay in place while the tablecloth (cupula) moves.
Understanding this distinction is crucial for choosing the appropriate Casani technique based on the likelihood of debris location and desired outcome.
Key Takeaways (Likely Short-Arm Debris)
The Casani maneuver's effectiveness for likely short-arm debris is directly tied to accurately identifying the affected ear.
Recent literature suggests that short arm debris is likely more common in apogeotropic horizontal canal BPPV due to sleeping habits.
Understanding the push-pull mechanics and their excitatory/inhibitory effects is crucial for optimal short-arm horizontal canal BPPV outcomes.
Clinicians should carefully consider the patient's presentation and choose the appropriate Casani technique.
In Part II, we will talk about the Casani Maneuver for long-arm disorders of the horizontal semicircular canal - stay tuned!
Disclaimer: This article is for informational purposes only and should not replace professional medical advice. Consult with a qualified healthcare professional for diagnosis and treatment of BPPV.