
THE HEAVE EIGENVECTOR: DECODING THE MATHEMATICAL AXIS OF MDDS BOBBING


Mal de Debarquement Syndrome (MdDS) is a clinical condition characterized by a persistent internal sensation of vertical oscillation, known as the “heave eigenvector”. This syndrome occurs when the “velocity storage mechanism” fails to reset following exposure to passive motion, requiring a targeted intervention that uses vertical “vection” to force a subcortical “neural dump” of the maladaptive signal. To resolve this “perseverating pattern”, clinicians must use high-intensity optokinetic flow to challenge the brain’s internal reference against the stable hardware of the “vestibular anchor” and “somatosensory anchor”.
Understanding the Heave Eigenvector as a Mathematical Coordinate
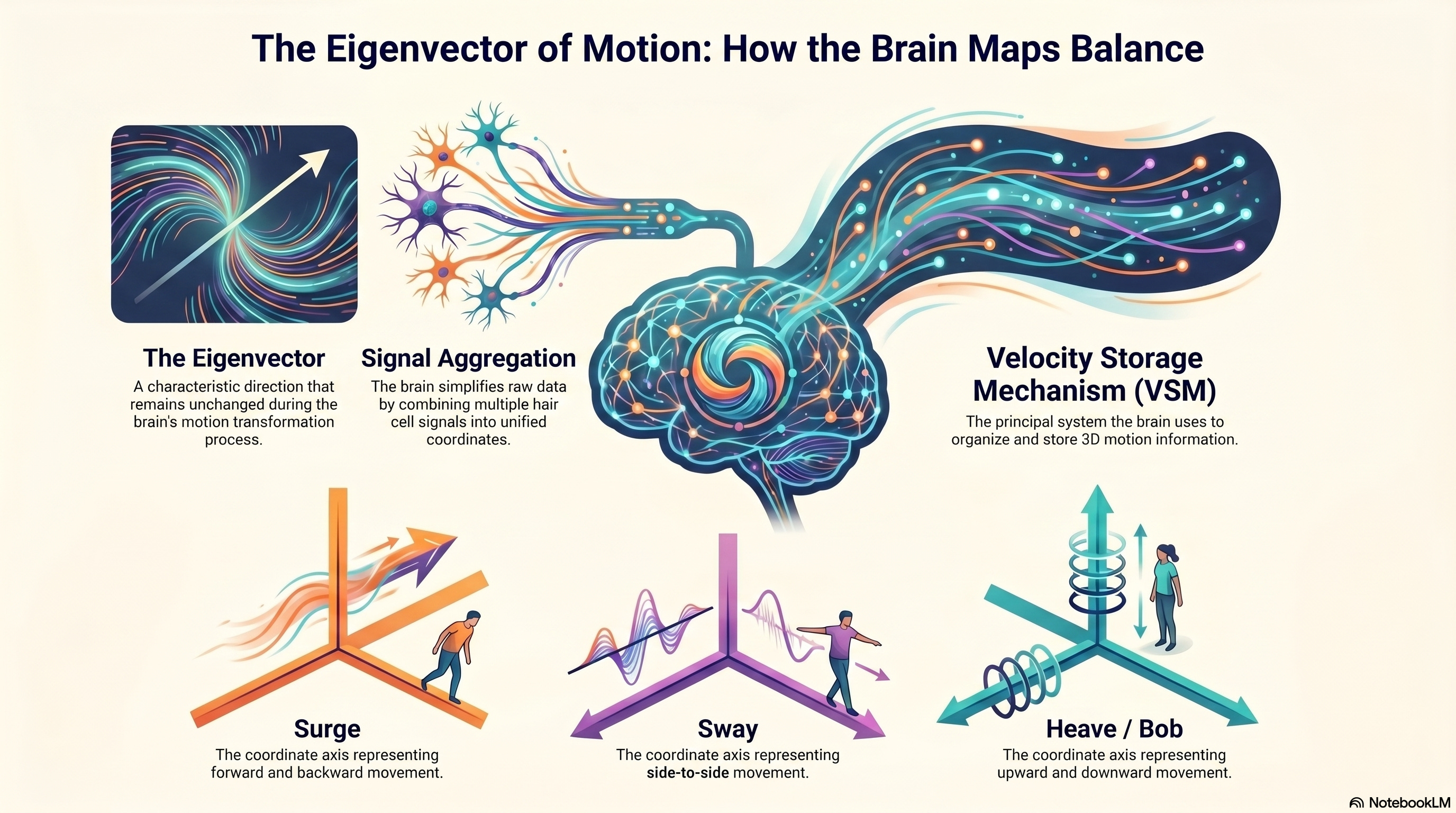
The “heave eigenvector” is not merely a sensation; it is the mathematical axis within the “velocity storage mechanism” (VSM) that represents vertical linear motion. The brain organizes spatial data into three primary coordinates: “surge” (forward/backward), “sway” (lateral), and “heave” (vertical). In a healthy terrestrial environment, this “heave eigenvector” remains silent unless the body is physically moving up or down.
However, when a patient is exposed to continuous passive motion—on a boat, train, or plane—the brain entrains to that oscillation. It builds an internal model that accepts constant heaving as the new spatial reality. Once the patient returns to stable ground, the brain fails to delete this model, continuing to project the “heave eigenvector” into the stationary world. This creates a “maladaptive sensory strategy” in which the brain is essentially asking, “Do I live on a boat, or do I not?” Because it cannot reconcile the difference, it persists in the bobbing rhythm.

The Supine/Sidelying Mechanism: Why Sleeping on a Boat Flips the Script
A critical nuance in MdDS is that it can develop even when a patient is sleeping. When the body is in a supine position, the orientation of the “sacculus” and “utriculus” relative to gravity shifts. In this “flipped” configuration, the “sacculus” and “utriculus” reorient their roles in detecting linear acceleration. While unconscious, the brain continues to receive constant data about the boat’s heave from these reoriented sensors.
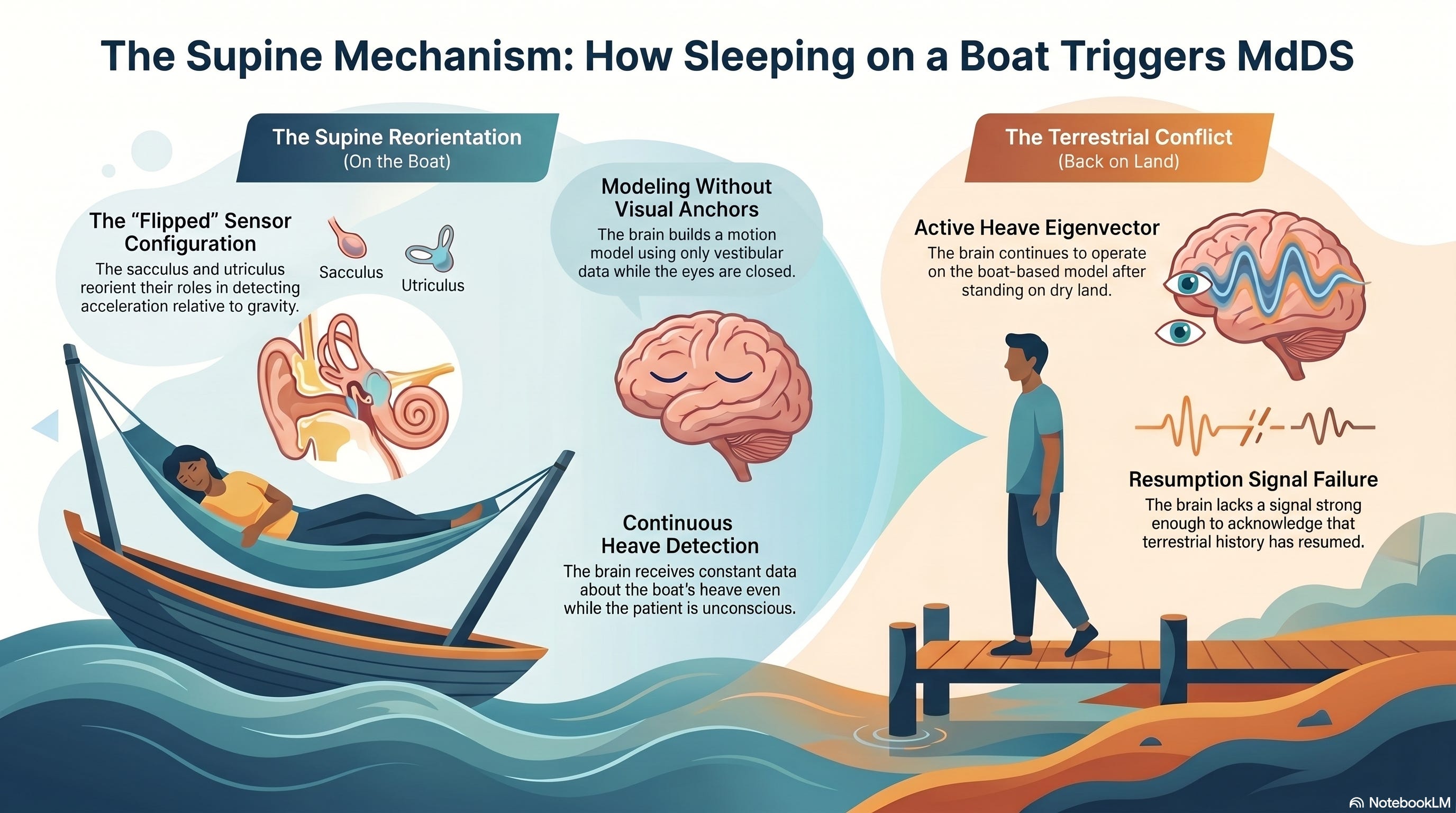
Without the visual system to provide a terrestrial anchor, the “velocity storage mechanism” relies entirely on this “flipped” vestibular and somatosensory data to build its motion model. When the patient finally stands up on dry land, the brain is still operating on the “supine-boat” model. The “heave eigenvector” remains active because the brain has not yet received a strong enough signal to acknowledge that its terrestrial history has resumed.
Vection and the Application of Visual Torque
To disrupt this loop, we must introduce “vection”, the subcortical illusion of self-motion triggered by a moving visual field. Using the “Linear Vertical Reset” protocol, we apply high-contrast vertical stripes across the patient’s 100% visual field.
When the stripes move from top to bottom, they induce an upward “vection”, creating the compelling illusion that the patient is rising. Conversely, a bottom-to-top flow induces a downward “vection”.
This is the application of “visual torque” to the subcortical brain. We are creating a state of controlled chaos that mimics the boat's random motion, but with one critical difference: we are doing so while the patient is physically anchored to the earth. This “retinal slip” forces the brain to decide: Should it continue to trust the internal, perseverating bobbing model, or should it discard that model in favor of the new, aggressive visual data?
The Master Anchors: Vestibular Hardware and Millions of Somatosensory Inputs
The “neural dump” of the “heave eigenvector” only occurs when the brain is provided with an undeniable “ground truth.” This is where the “vestibular anchor” and “somatosensory anchor” provide the definitive tie-breaker.
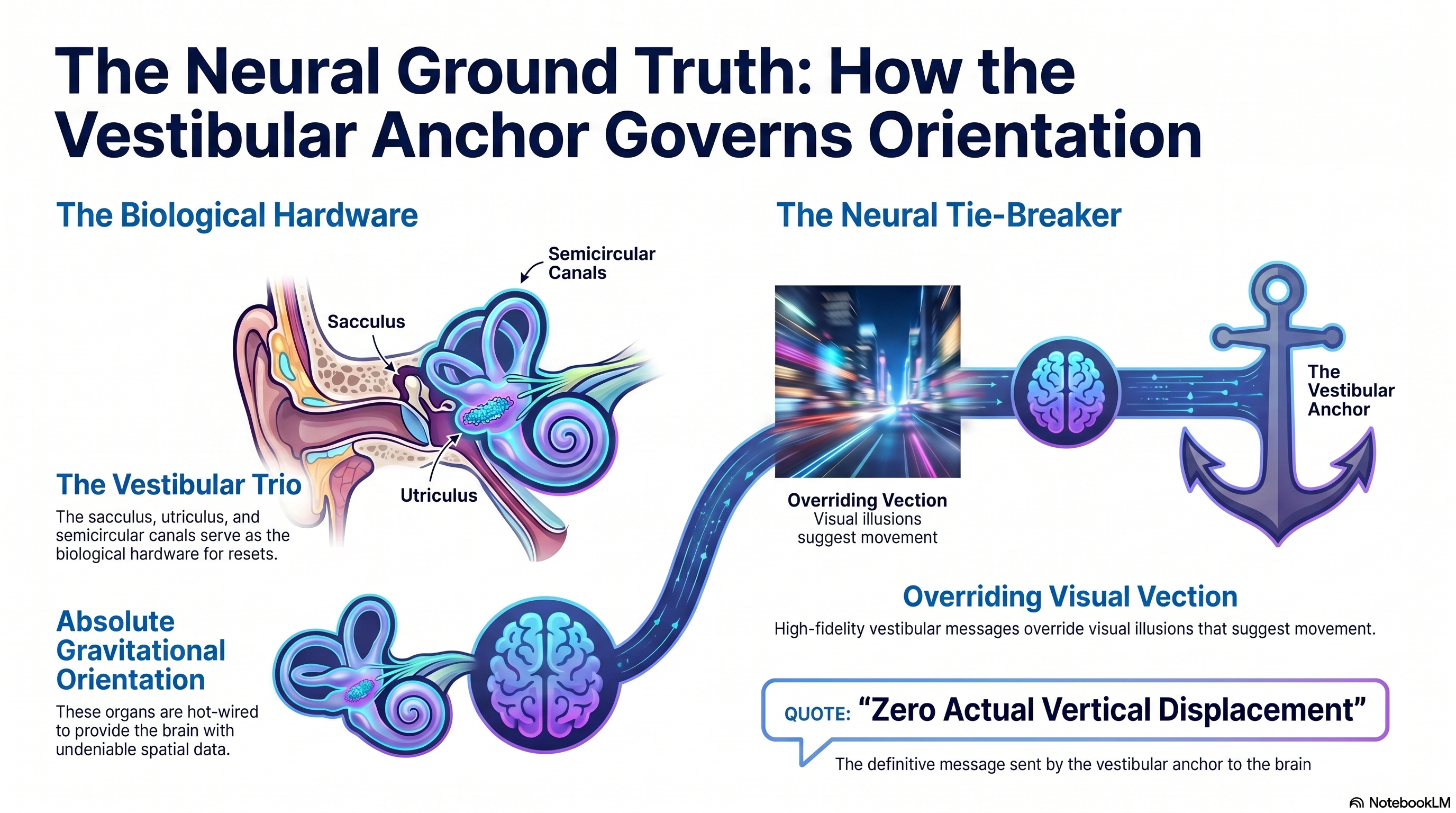
The “vestibular anchor” is the biological hardware of the reset. The “sacculus”, “utriculus”, and “semicircular canals” are hot-wired to provide the brain with absolute gravitational orientation. Even as the visual system induces “vection”, these organs are sending a high-fidelity message:
“There is zero actual vertical displacement.”
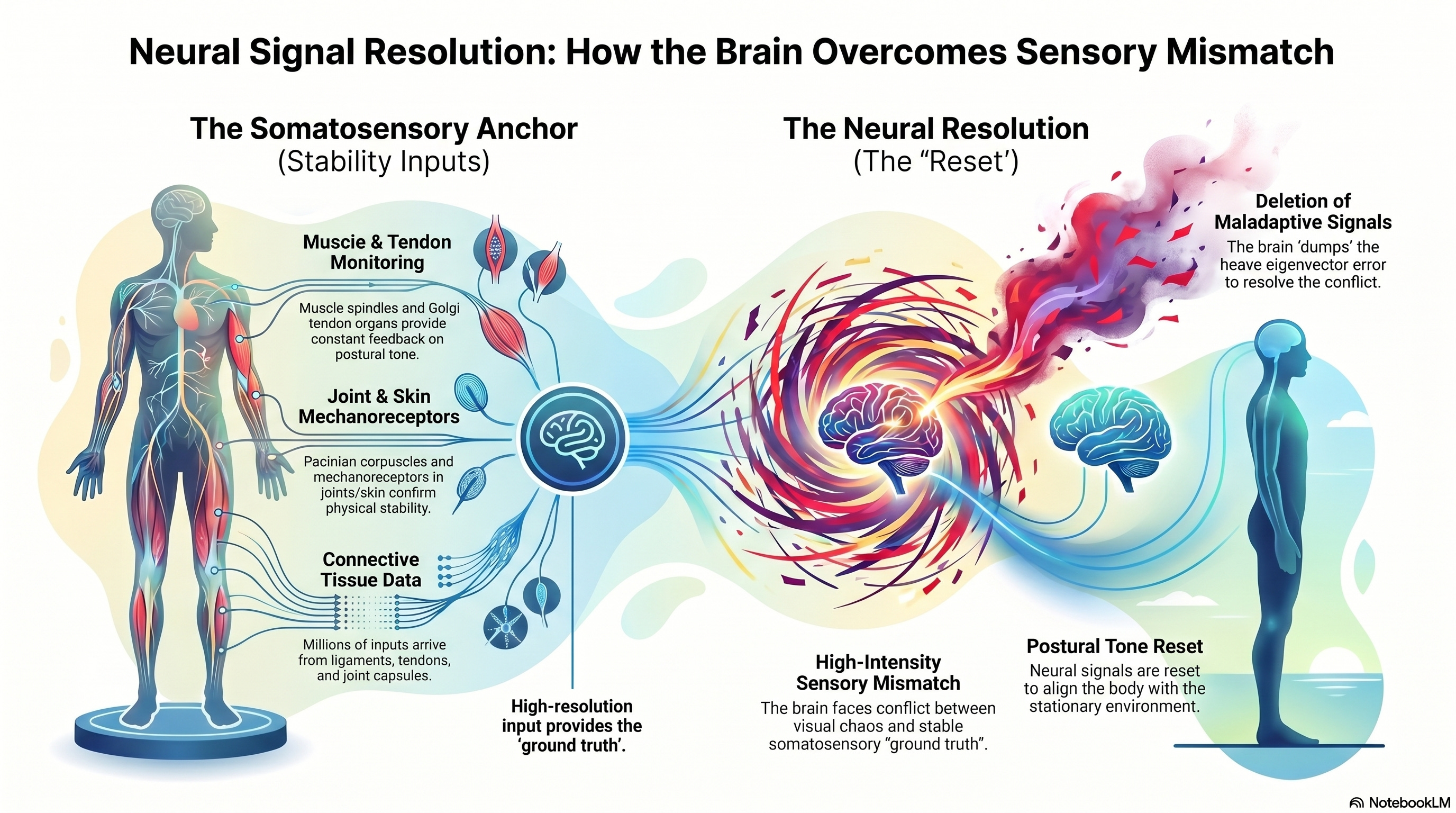
Simultaneously, the “Somatosensory Anchor” provides millions of inputs confirming stability. This includes:
“Muscle spindles” and “Golgi tendon organs” monitor postural tone.
“Pacinian corpuscles” and “mechanoreceptors” in the skin and joints.
Sensory data from “ligaments”, “tendons”, and “joint capsules”.
When the brain is trapped in the state of high-intensity “sensory mismatch” between the visual chaos and these stable anchors, it reaches a point of physiological decision. Faced with the overwhelming “ground truth” from the vestibular hardware and the millions of somatosensory signals from the feet and seat, the brain chooses to “dump” the maladaptive signal. It deletes the “heave eigenvector” error and resets the postural tone to match the stationary environment.
Clinical Application of Sensory Integration Method
To “optimize” the results of this reset, the professional must ensure the patient is in a weight-bearing, seated position. This ensures both the “vestibular anchor” and “somatosensory anchor” are fully engaged.
Use a “Flow Speed” of 10–20 and a “Bar Density” of 6–12 to induce sufficient “vection” to challenge the internal model.
Direct the patient to focus on the “Red Arrow” anchor, which serves as a static coordinate reference against the moving stripes.
Incorporate a “Washout Phase” between sets to allow the brain to process the signal integration and confirm the “dump.”
By “heaving” the patient through their vision while their body remains anchored, we “facilitate” the brain’s ability to abandon its “boat reality” and return to terrestrial stability.
Clinical References
Dai, M., Cohen, B., Cho, C., Shin, S., & Yakushin, S. B. (2014). Treatment of the Mal de Debarquement Syndrome: A 1-Year Follow-up. Frontiers in Neurology, 5, 124. DOI: 10.3389/fneur.2014.00124
Mucci, V., et al. (2018). Cumulative Experience of Mal de Debarquement Syndrome Patients Who Completed the Vestibular-Ocular Reflex Protocol. Frontiers in Medicine, 5, 175. DOI: 10.3389/fmed.2018.00175
Yakushin, S. B., et al. (2017). Orientation of the spatial vertical by the velocity storage mechanism. Journal of Neurophysiology, 118(4), 2000-2012. DOI: 10.1152/jn.00100.2017
Yuan, H., & Brennan, K. C. (2020). Functional Connectivity in Mal de Debarquement Syndrome: The Role of the Velocity Storage Mechanism. PNAS, 117(15), 8560-8568. DOI: 10.1073/pnas.1916325117