
The Oslerian Paradigm: Decoding the Sensory Strategy Beyond the Diagnosis of Dizziness

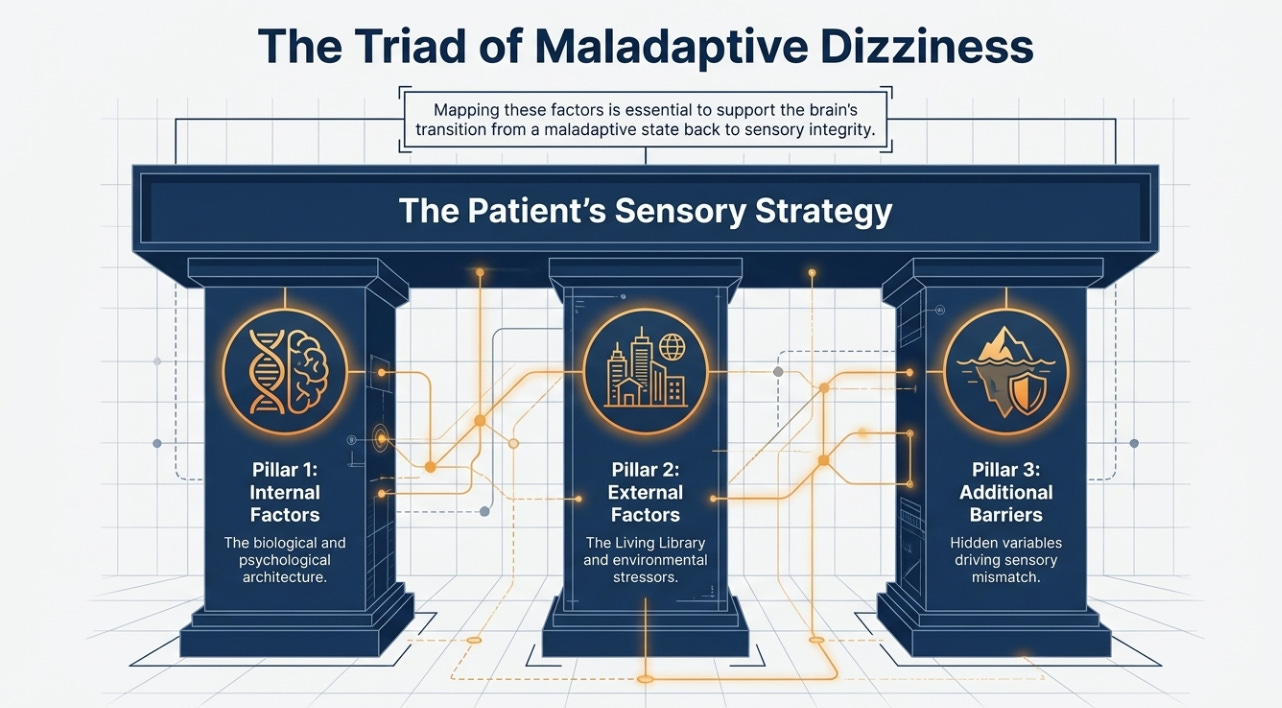
Oslerian principles define clinical excellence by integrating rigorous scholarship with a humanistic approach to patient care, prioritizing the “clinical gaze” to see the whole person. In vestibular rehabilitation, these principles require the clinician to move beyond the “balkanization” of medical subspecialties—where practitioners focus only on a localized condition—to understand the internal and external drivers of a patient’s sensory strategy. By mapping these factors, professionals support the brain’s transition from a maladaptive state to one of sensory integrity.
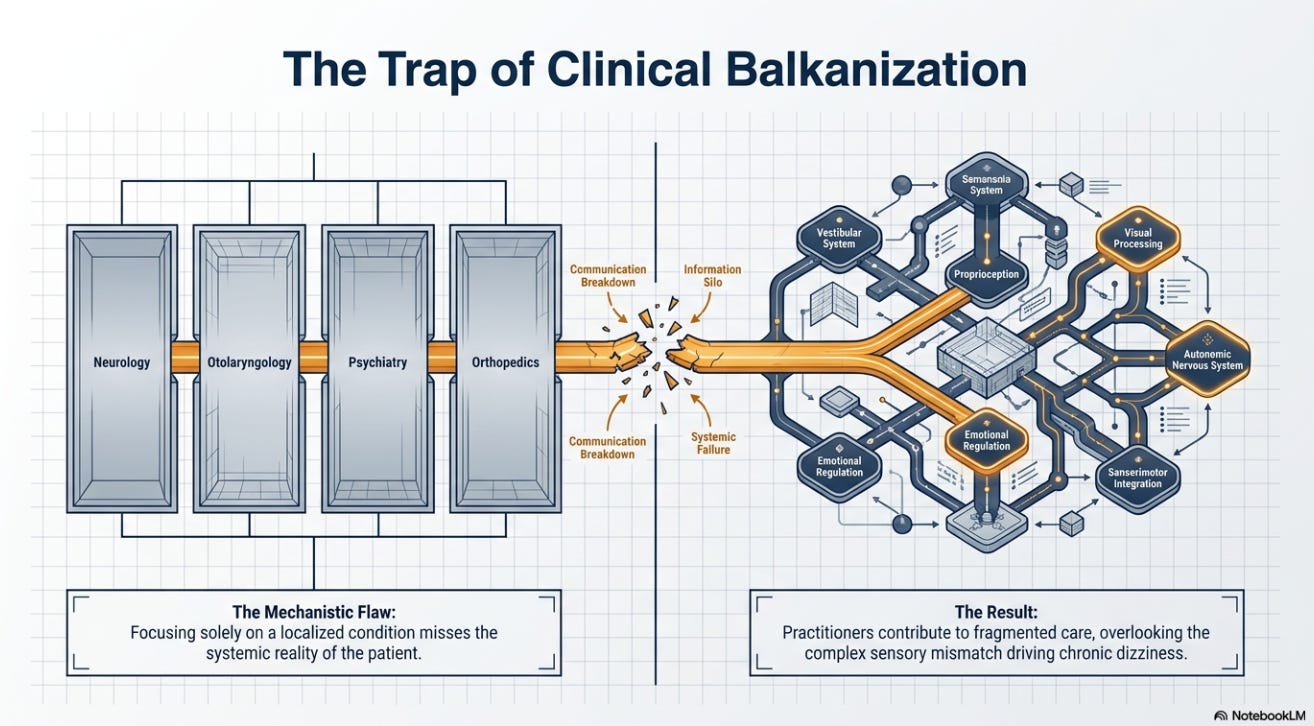
HOW DOES THE BEDSIDE TRADITION PREVENT CLINICAL BALKANIZATION?
Sir William Osler, the prototype of the modern physician, argued that the integration of scholarship with patient care was central to the “science and art of medicine.” As noted by Geyman (1983), Osler taught by example and was as concerned with the ideals of medicine as with its technical knowledge. In the context of the dizzy patient, this means rejecting a purely mechanistic view of pathology. When a vestibular professional focuses solely on a “condition,” they contribute to the “balkanization” of care, often overlooking the complex sensory mismatch that shapes the patient’s functional reality.
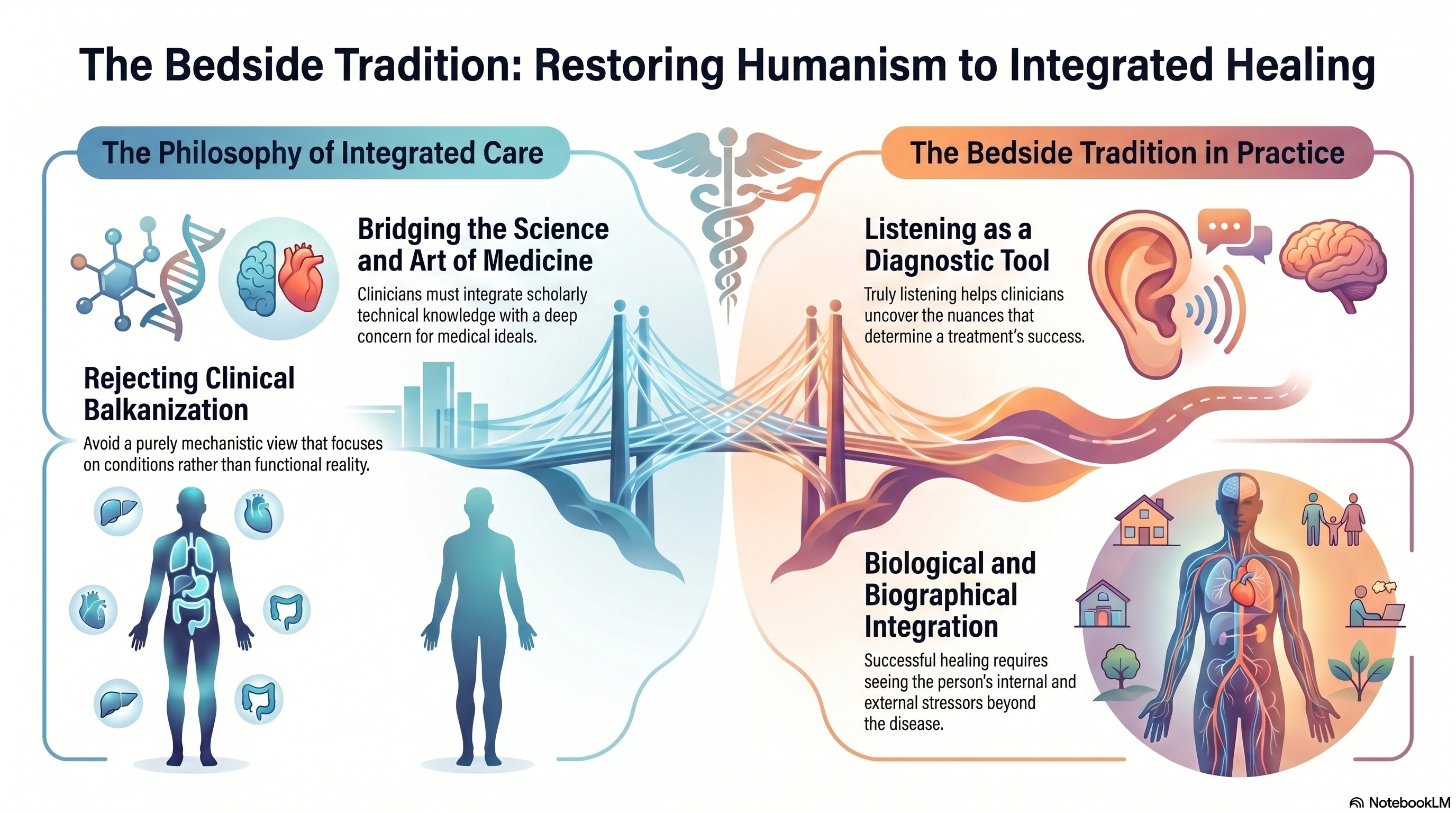
This humanistic foundation is also a central theme for Dr. Daniel Flora, an oncologist who identifies the “bedside manner” as a primary diagnostic tool. While oncology and vestibular science manage different biological systems, the requirement to see the person beyond the disease is identical. Dr. Flora’s work on “Curative” emphasizes that when a clinician truly listens, they uncover the biological and biographical nuances—the internal and external stressors—that dictate whether a treatment plan succeeds or fails.
WHAT INTERNAL FACTORS SHAPE THE PATIENT’S SENSORY SIGNATURE?
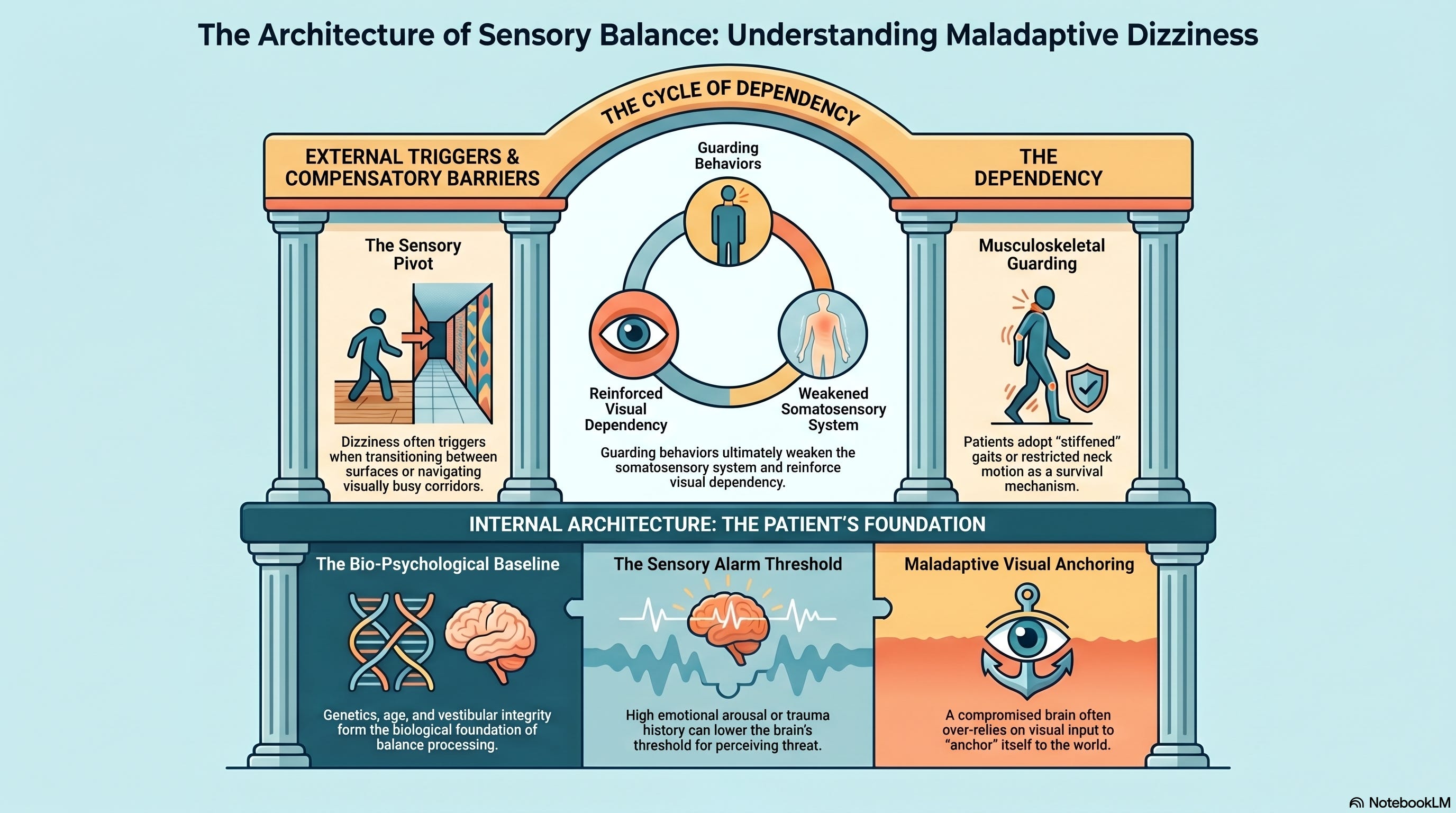
Internal factors encompass the biological and psychological architecture that the patient brings to the clinic. When clinicians follow the Oslerian rule to “listen to your patient,” they identify the biological baseline, including age, genetics, and the integrity of the vestibular and somatosensory systems. These elements form the foundation of the brain's balance processing.
However, the psychological architecture is equally critical. Factors such as emotional regulation, attention, and learned behaviors determine the threshold at which the brain perceives a sensory signal as a threat. A patient with high emotional arousal or a history of trauma may experience a lower “sensory alarm” threshold, forcing the brain to adopt a strong visual component to “anchor” itself to the world. Understanding these internal drivers allows the professional to address the root of the maladaptive strategy rather than just the symptom of dizziness.
HOW DO EXTERNAL FACTORS TRIGGER A MALADAPTIVE STRATEGY?
The brain does not process balance in a vacuum; it operates within a physical and social environment. Oslerian medicine demands that we observe the patient in their “living library”—the world they navigate daily. External factors include the physical surroundings, social demands, and occupational pressures. Dizziness often emerges during a “sensory pivot,” such as transitioning from a firm surface to a compliant one or navigating a “visually busy” corridor.
When the environment becomes too complex, a brain with compromised signaling must choose which sensory inputs to trust. This often results in a surface-level or visual dependency, in which the patient relies on one system to compensate for the perceived failure of another. By observing the patient’s interaction with their environment, the clinician identifies the external stressors that force the brain into a state of sensory mismatch.
WHY MUST WE IDENTIFY ADDITIONAL FACTORS IN CHRONIC DIZZINESS?
A standard diagnosis often overlooks the additional factors that cloud the clinical picture and reinforce instability. These variables include musculoskeletal guarding, medication effects, and the presence of learning or attention disorders. Many patients adopt a “stiffened” gait or restrict cervical motion as a survival mechanism to avoid triggering vertigo.
While this musculoskeletal guarding offers a temporary sense of security, it ultimately compromises the integrity of the somatosensory system and reinforces the brain’s reliance on a strong visual component. By identifying these additional factors during the evaluation, the vestibular professional can coordinate a plan that removes these barriers. We use targeted interventions to optimize the signaling environment, thereby enabling the brain to once again prioritize reliable vestibular data over noisy, maladaptive inputs.
References
Flora, D. (2026). Curative. Substack.

Geyman, J. P. (1983). The Oslerian tradition and changing medical education: A reappraisal. The Western Journal of Medicine, 138(6), 884–888. https://pubmed.ncbi.nlm.nih.gov/6351442/
John, M. (2013). From Osler to the cone technique. HSR Proceedings in Intensive Care & Cardiovascular Anesthesia, 5(1), 57–58. https://pubmed.ncbi.nlm.nih.gov/23734290/
Scambler, G. (2000). Sir William Osler, MD. AMA Journal of Ethics. https://journalofethics.ama-assn.org/article/sir-william-osler-md/2000-01