
The Post-Concussion Energy Crisis: Why the Vestibular Nerve Is a Key Target


A concussion, or mild traumatic brain injury (mTBI), fundamentally changes the way the brain works. For too long, people viewed a concussion as a microscopic bruise. This perspective overlooks the central physiological truth: a concussion triggers a metabolic crisis that creates an energy deficit throughout the entire nervous system. Understanding this cellular-level event is crucial for effective treatment.
The Neurometabolic Cascade
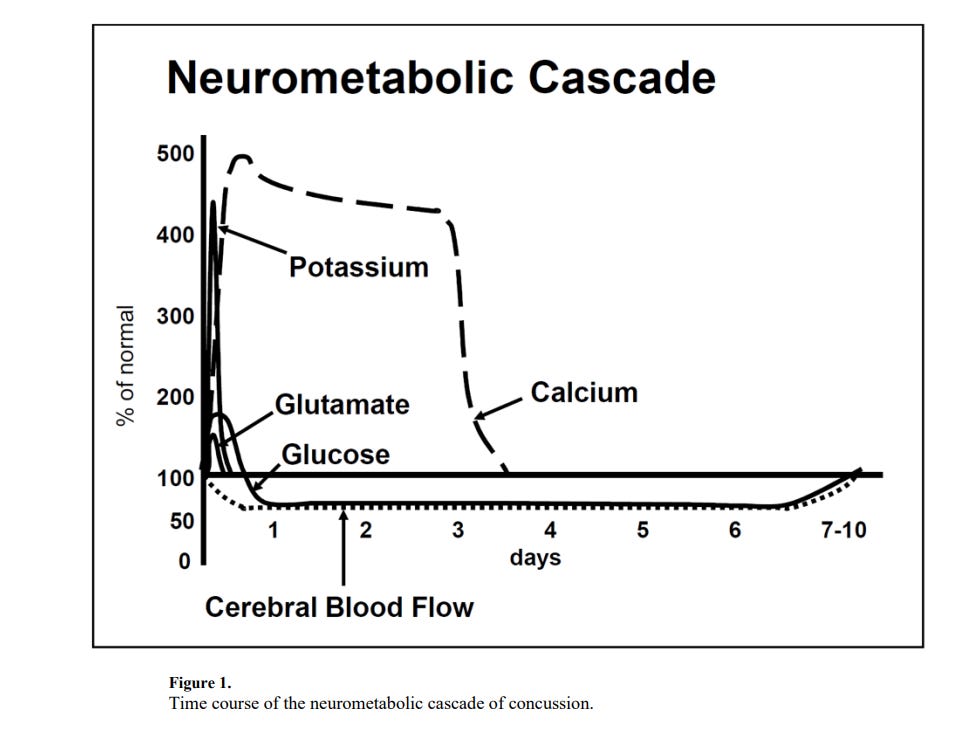
The definitive model that explains post-concussion symptoms is the Neurometabolic Cascade, as famously illustrated by Giza & Hovda in 2014. This cascade begins the moment a biomechanical force, such as a rotational or shear injury, impacts the brain. This initial mechanical trauma triggers massive, widespread ionic shifts.
The most prominent shifts include a rapid efflux of potassium ions (K+) out of the nerve cell and a large influx of calcium ions (Ca2+) into the cell. This disequilibrium forces the cell’s ion pumps—specifically the Sodium-Potassium ATPase—into immediate, desperate ‘hyperdrive‘ to restore the resting membrane potential.
The pumps consume adenosine triphosphate (ATP) at a frantic, unsustainable pace to drive the ions back across the cell membrane. This excessive activity results in a rapid and profound depletion of intracellular ATP, creating what researchers refer to as an ‘energy crisis‘.
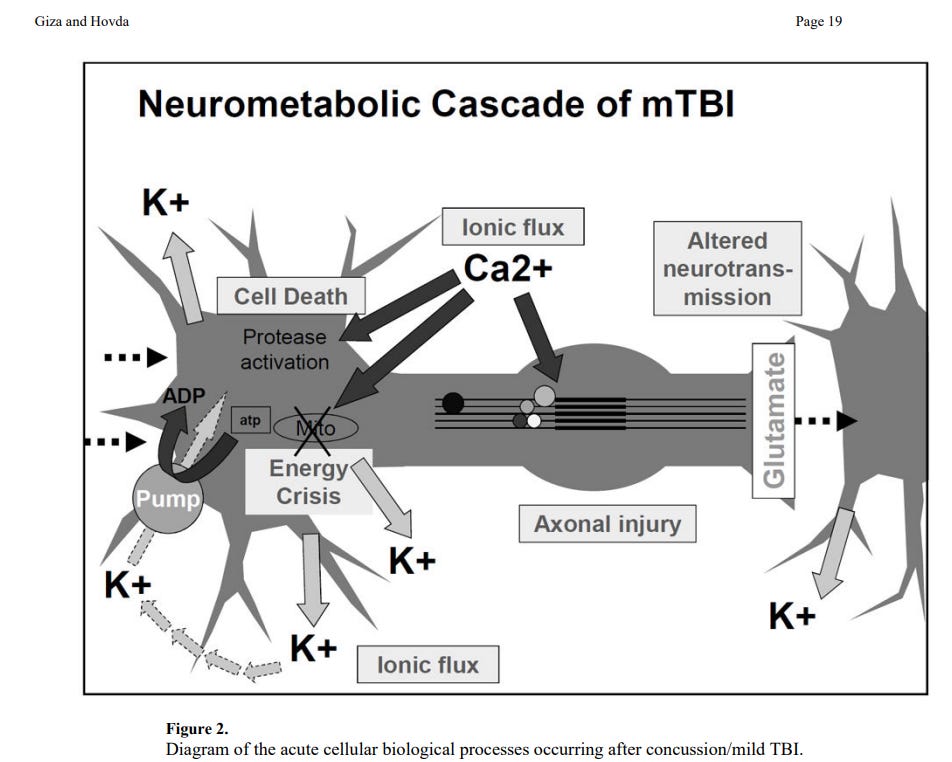
In a seemingly paradoxical move to feed this ATP-starved system, the brain shifts to excessive glycolysis, leading to an initial period of hyperglycemia followed by lactic acid accumulation. Furthermore, excitatory neurotransmitters like glutamate release, coupled with abnormal ion fluxes and impaired glucose metabolism, severely alter cerebral blood flow (CBF). This is a critical point: the brain experiences a state of increased metabolic demand (it needs energy immediately) but simultaneously suffers from reduced blood flow (it cannot get the necessary oxygen and glucose), effectively starving the cells and prolonging the energy crisis.
The Axonal and Vestibular Connection
This metabolic and ionic stress not only impacts the large axons within the brain but also equally damages the delicate and exposed microstructures of the peripheral nervous system. This is where the vestibular system comes into play.
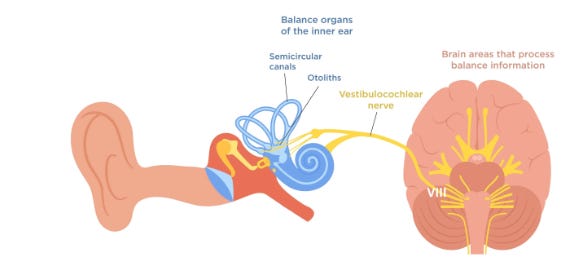
The vestibular nerve (Cranial Nerve VIII) transmits balance and spatial orientation information from the inner ear to the brainstem. Like the axons in the brain, the axons of the vestibular nerve and the microstructures of the vestibular ganglia are highly vulnerable to the same biomechanical shear forces that cause the initial concussion.
The Biomechanical Vulnerability
The anatomy of the vestibular nerve exacerbates this vulnerability. The inner ear’s bony labyrinth, which houses the vestibular apparatus, is located ‘peripheral to the brain’s center of mass‘. This peripheral location acts like a ‘lever arm‘ during rapid head acceleration and deceleration (the mechanism of concussion). As the skull twists and shears, the resulting forces exert significant ‘tension and shear strain‘ directly on the fragile vestibular nerve as it stretches between the inner ear and the brainstem. This anatomical reality means that the vestibular nerve is subjected to extreme biomechanical stress, potentially making it one of the most vulnerable neural structures to the initial traumatic event.
The same ‘ionic shifts‘ and ‘ATP depletion‘ that occur in the cerebral cortex are also possible along the entire length of the vestibular nerve and within the specialized neural tissue of the inner ear. Damage to these peripheral vestibular structures can manifest as:
Axonal Injury: Traumatic stress can cause microscopic damage to the vestibular nerve’s axons, disrupting the precise timing and fidelity of balance signals sent to the brain.
Microstructure Damage: The metabolic cascade may compromise the surrounding Schwann cells or even the delicate hair cell connections within the ampullae of the semicircular canals. This damage directly interferes with the inner ear’s ability to accurately detect head motion.
Clinical Relevance and Chronic Pathophysiology
The sustained metabolic dysfunction—the Chronic Pathophysiology—is what drives persistent post-concussion syndrome (PCS). The Giza & Hovda model clearly delineates how the acute crisis transitions into chronic clinical issues:
Ion Changes → Sensory Hypersensitivity: The initial ionic shifts lead to neuronal irritability that contributes directly to common sensory overload symptoms, such as ‘migraines‘, ‘photophobia‘ (light sensitivity), and ‘phonophobia‘ (sound sensitivity). This neurological over-reaction forces patients into avoidance behaviors, slowing recovery.
Energy Crisis → Vulnerability: The brain and nervous system remain in a state of prolonged energy depletion. This means that a second impact, even a minor one, is significantly more dangerous because the cells lack the energetic resources to cope, making the system extremely vulnerable to second injury.
Axonal Injury & Neurotransmission → Cognitive Deficits: Microscopic axonal injury, combined with altered neurotransmission (particularly of glutamate), impairs the efficient communication between neurons. Clinically, this translates to tangible cognitive and processing issues, including ‘impaired learning‘, ‘reduced cognition‘, and ‘slowed reaction time‘.
Therefore, many persistent post-concussion symptoms—such as dizziness, gaze instability, and imbalance—are not solely due to damage to the central balance centers of the brain. They are often a direct result of the metabolic cascade’s impact on the peripheral vestibular nerve, an injury that creates a lasting deficit in the body’s primary balance sensor.
To treat a patient effectively, clinicians must acknowledge that a concussion is an energy crisis affecting the entire system, including the vulnerable vestibular nerve. They must structure rehabilitation to allow for metabolic recovery and functional re-training of the damaged circuits.