
The Sensory Reweighting Solution to the Automobile Effect: Overriding Mal de Debarquement Syndrome via Multimodal Masking
The AUtomobile Response

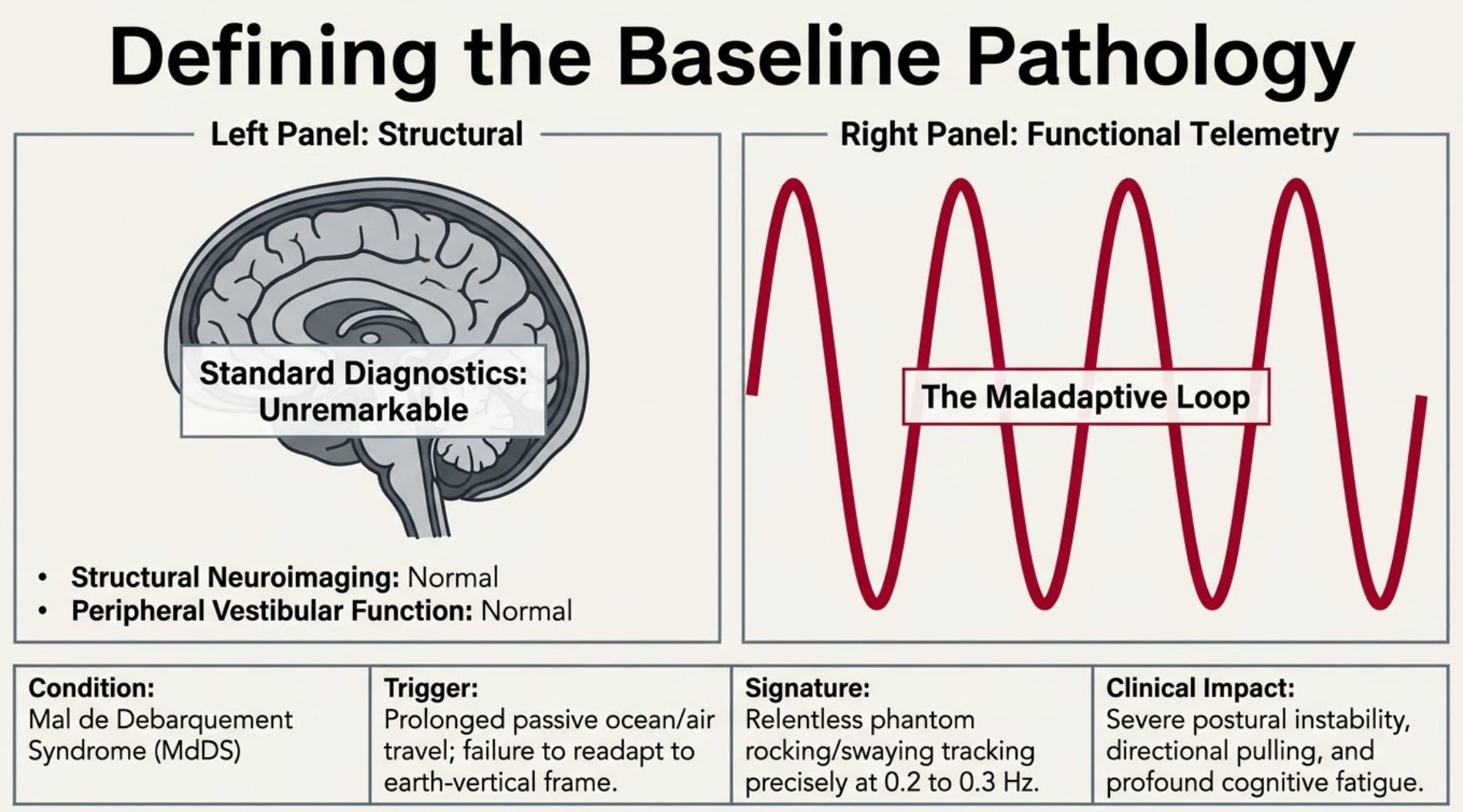
Mal de Debarquement Syndrome (MdDS) is a motion-induced central vestibular disorder characterized by a persistent, phantom sensation of rocking, swaying, or bobbing, typically tracking at a highly conserved frequency of 0.2 to 0.3 Hz. This debilitating condition primarily arises after prolonged exposure to passive ocean or air travel, resulting in an internal spatial mismatch where the central nervous system fails to readapt to a stable earth-vertical frame of reference. While standard structural neuroimaging and peripheral vestibular diagnostics routinely return completely normal, the condition drives severe postural instability, a subjective sensation of directional pulling, and profound cognitive fatigue.
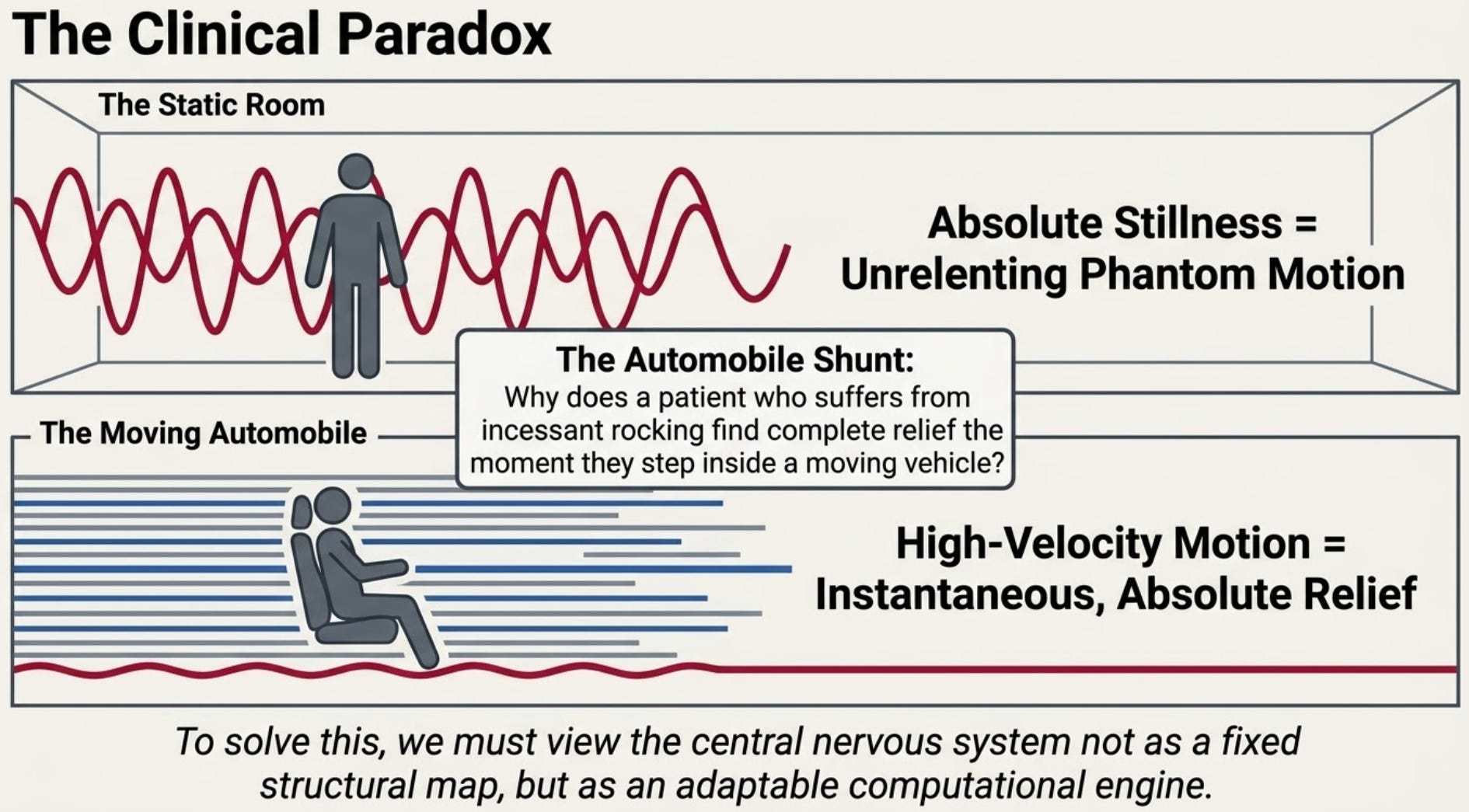
When managing individuals with classic MdDS, vestibular specialists routinely encounter a striking clinical paradox:
A patient who suffers from an incessant, phantom sensation of rocking or swaying will find absolute, instantaneous relief the moment they step inside a moving automobile.
While traditional mathematical and neurophysiological models attribute this to a computational re-zeroing of the brainstem’s velocity storage integrator, a more direct and clinically actionable explanation exists. By analyzing this phenomenon through a sensory strategy approach, the temporary cessation of MdDS symptoms can be explained by dynamic sensory reweighting and simultaneous multimodal masking.
What is the Sensory Strategy Approach to the Automobile Shunt?
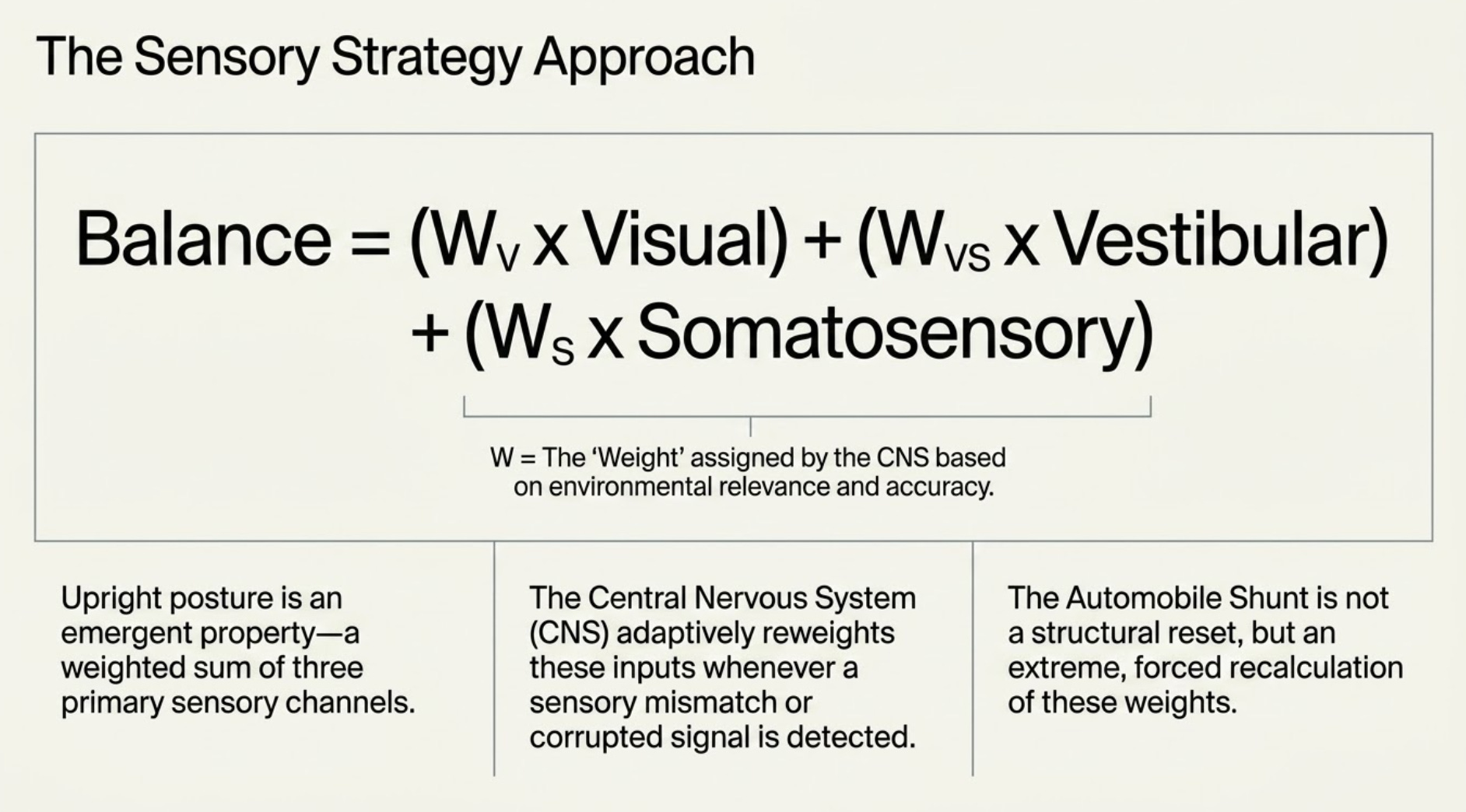
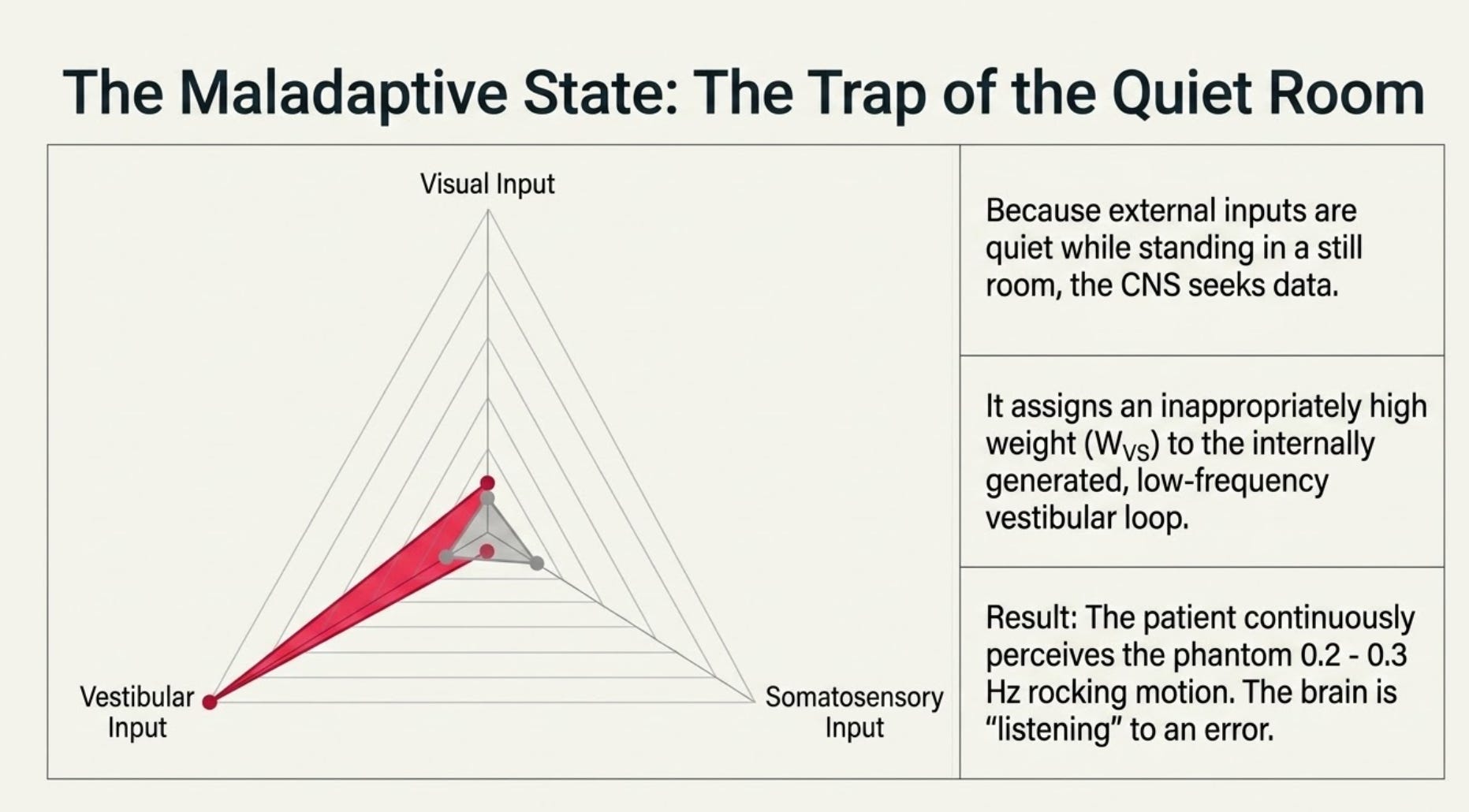
The emergent control of upright posture and balance is a weighted sum of visual, vestibular, and somatosensory inputs. Under the sensory weighting hypothesis, the central nervous system multiplies each sensory channel by a specific weight based on its environmental relevance and accuracy, adaptively reweighting these inputs whenever a sensory mismatch or corrupted signal is detected (Jeka et al., 2008).
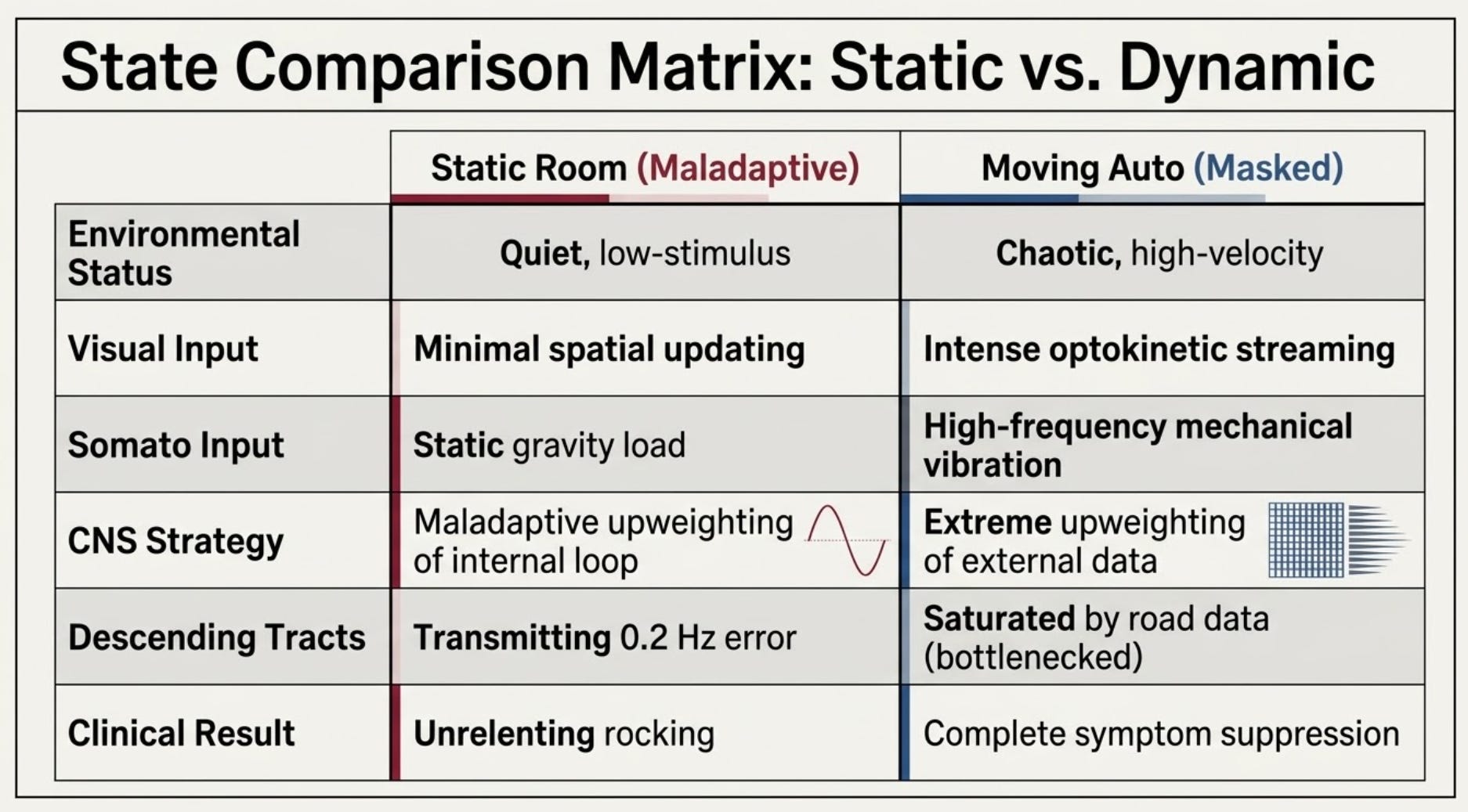
In a static environment, a patient with active MdDS utilizes a maladaptive sensory strategy. Because external inputs are quiet while standing in a still room, the central nervous system assigns an inappropriately high weight to an internally generated, low-frequency vestibular loop, causing the patient to continuously perceive a phantom rocking motion at 0.2 Hz or 0.3 Hz.
When the patient enters a moving vehicle, the automobile functions as a real-world simulator that forces a rapid, profound rearrangement of this sensory hierarchy. Instead of addressing the internal error directly, the moving vehicle simultaneously introduces an overwhelming avalanche of high-amplitude, high-frequency external data across multiple sensory channels.
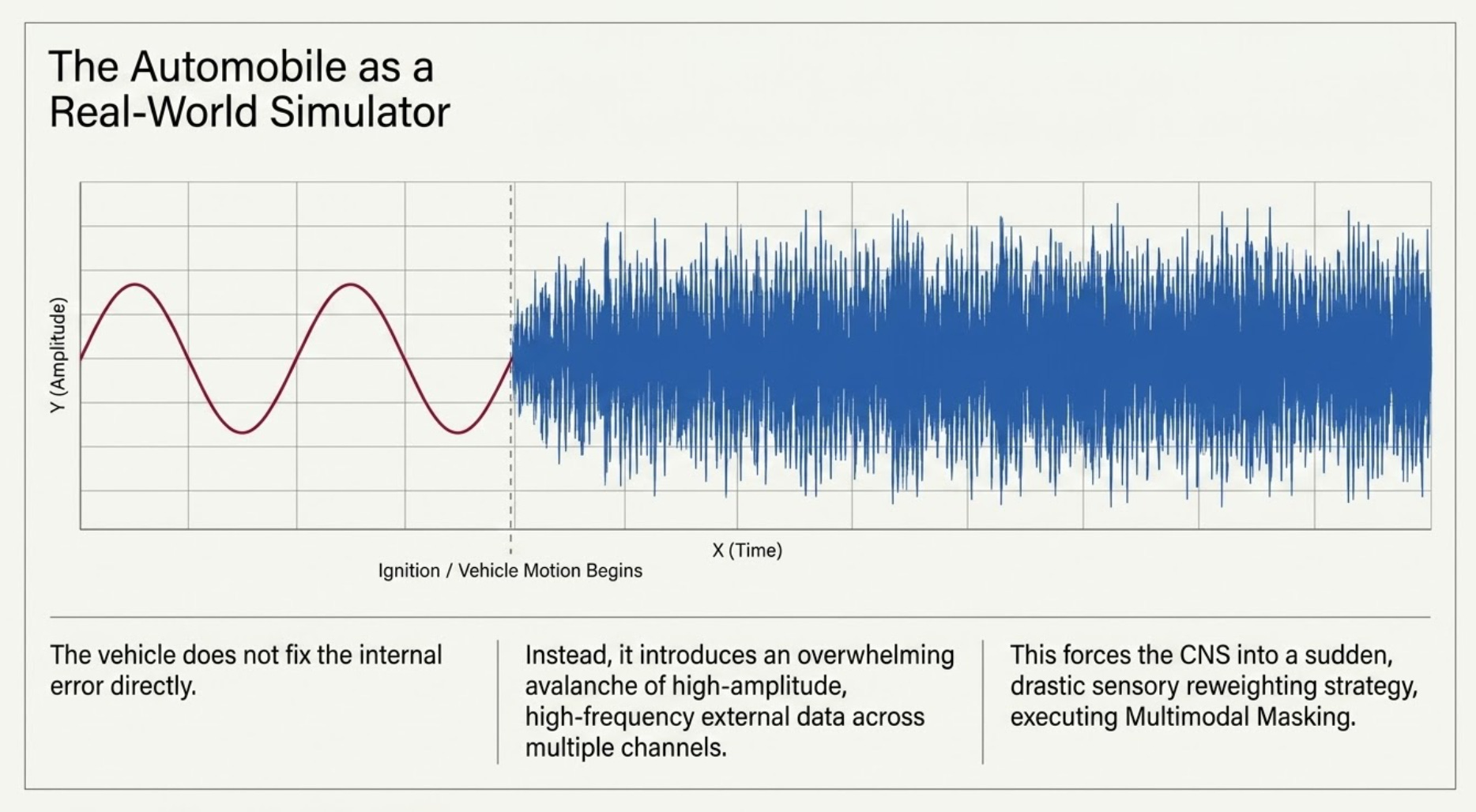
This immense external signal effectively masks the low-frequency internal reference, forcing the central nervous system to undergo a sudden, drastic reweighting of sensory inputs.
How Do Dual Sensory Channels Execute the Overriding Shunt?
The reason the automobile effect delivers such complete, instantaneous relief—where simpler activities like walking down a hallway fail—is that it imposes a strong visual and somatosensory component simultaneously. These two systems are overdriven in complete congruence, forcing the central nervous system to down-weight the corrupted internal vestibular reference.
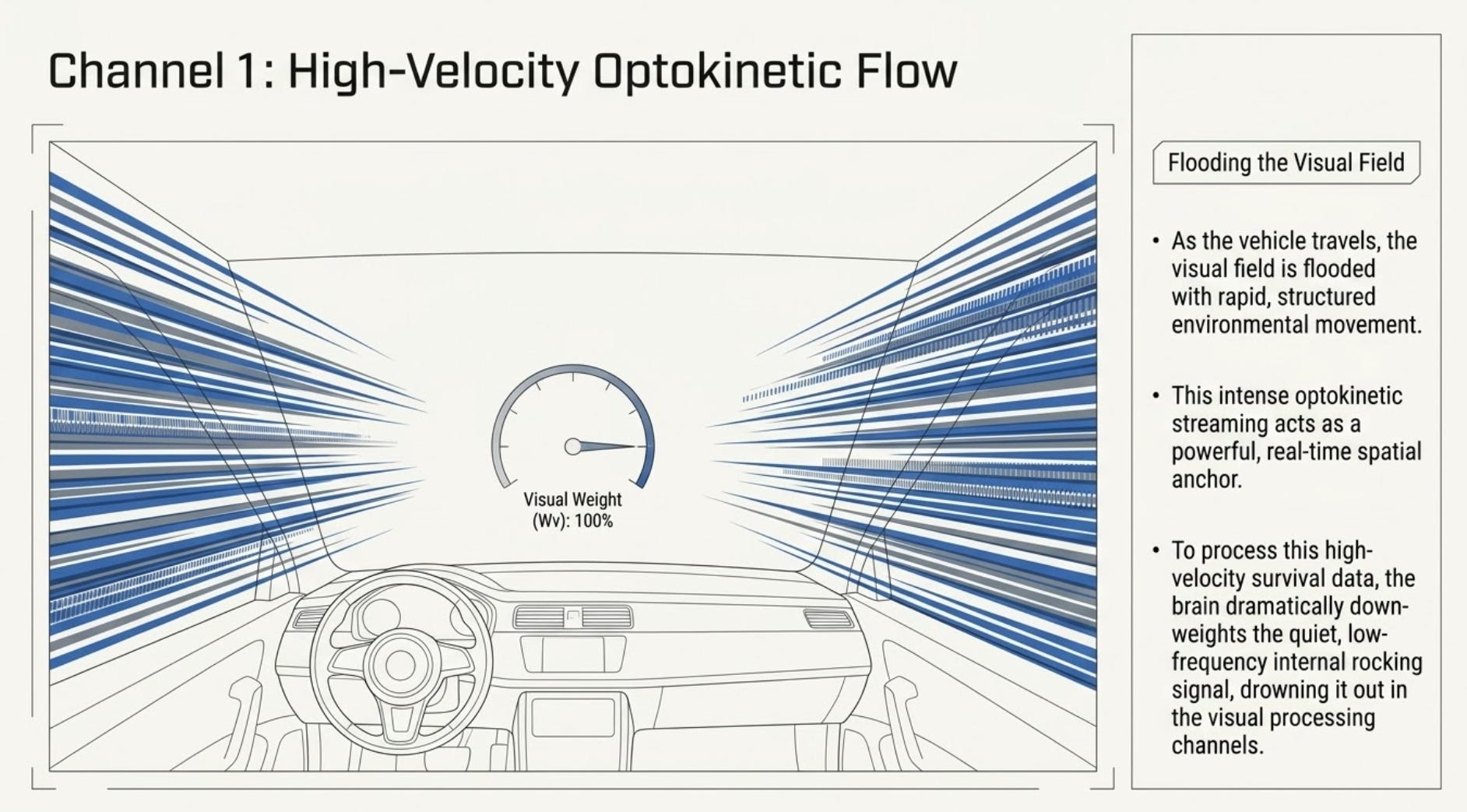
The strong visual component is driven by high-velocity optokinetic flow. As the vehicle travels forward, the patient’s visual field is flooded with rapid, structured environmental movement. This intense optokinetic streaming acts as a powerful external signal that commands the central balance network. Because the brain must process this high-velocity, real-time visual motion to maintain spatial awareness, it dramatically down-weights the quiet, low-frequency internal rocking signal, effectively drowning it out in the visual processing channels.
Concurrently, the strong somatosensory component delivers an equal level of physical stabilization.
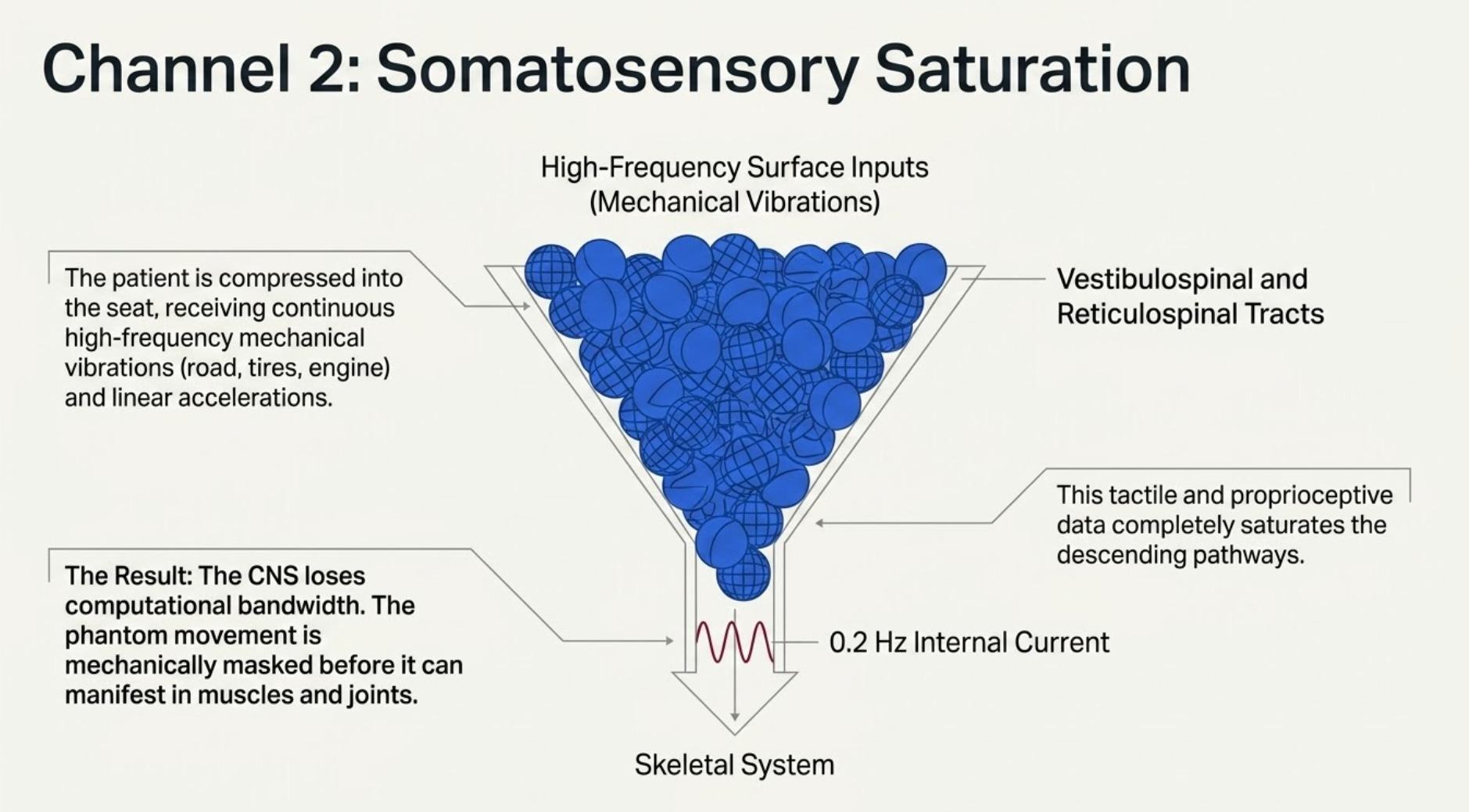
The patient is compressed into the automobile seat, receiving a continuous stream of high-frequency mechanical vibrations from the road, tires, and engine, alongside real-time linear accelerations.
This continuous tactile and proprioceptive data completely saturates the vestibulospinal and reticulospinal tracts. Because these pathways are entirely occupied by high-frequency surface inputs, the central nervous system lacks the computational bandwidth to transmit the slow, low-frequency (0.2 Hz) internal current to the skeletal system.
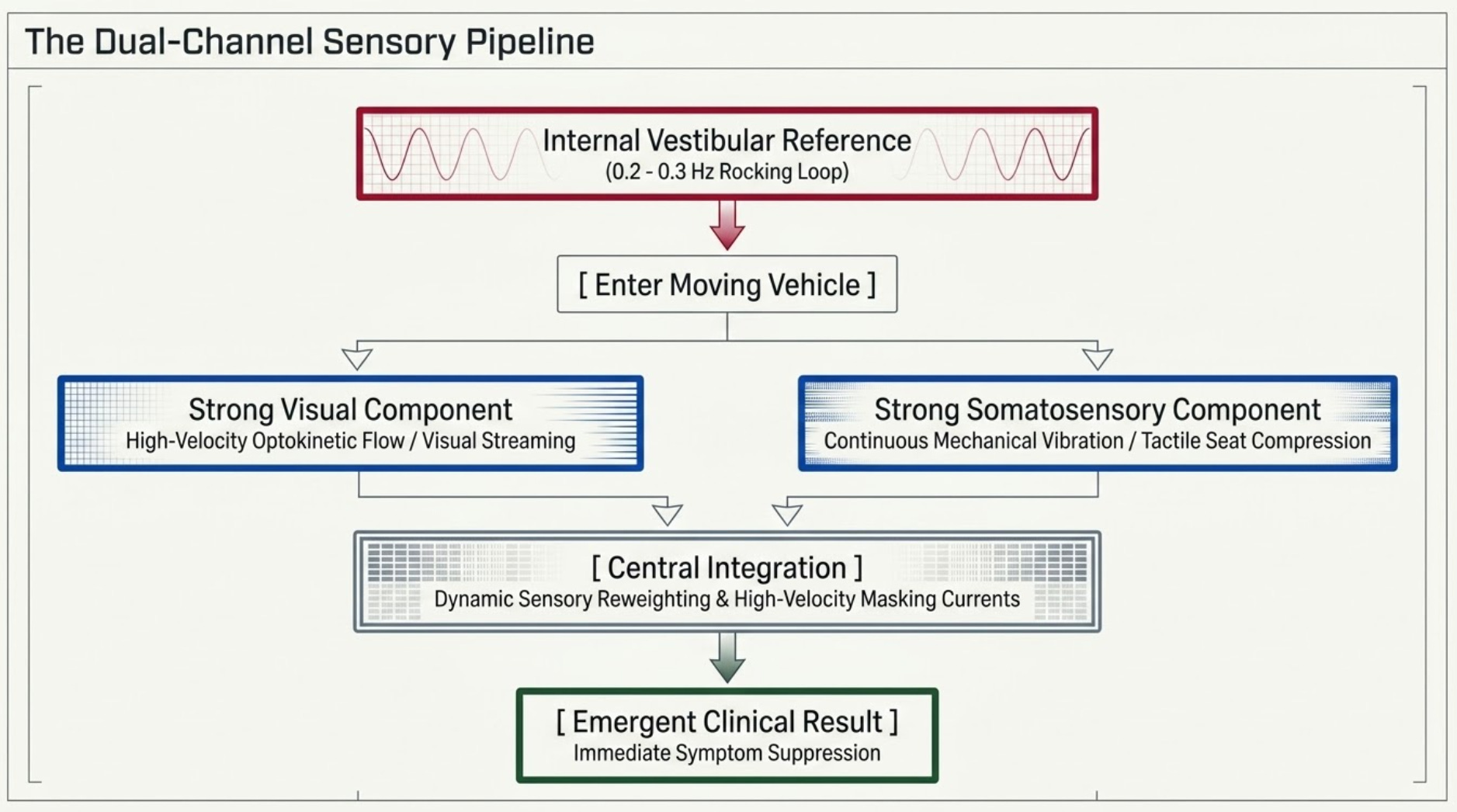
The phantom movement is masked before it can ever manifest in the muscles and joints.
Why Does the Post-Drive Collapse Occur?
This sensory strategy approach perfectly explains the immediate post-drive collapse—the instantaneous return of rocking the moment the vehicle stops. Because this phenomenon relies entirely on sensory masking via dynamic reweighting rather than a structural, long-term adaptation of the underlying vestibular pathways, the relief is strictly stimulus-dependent.
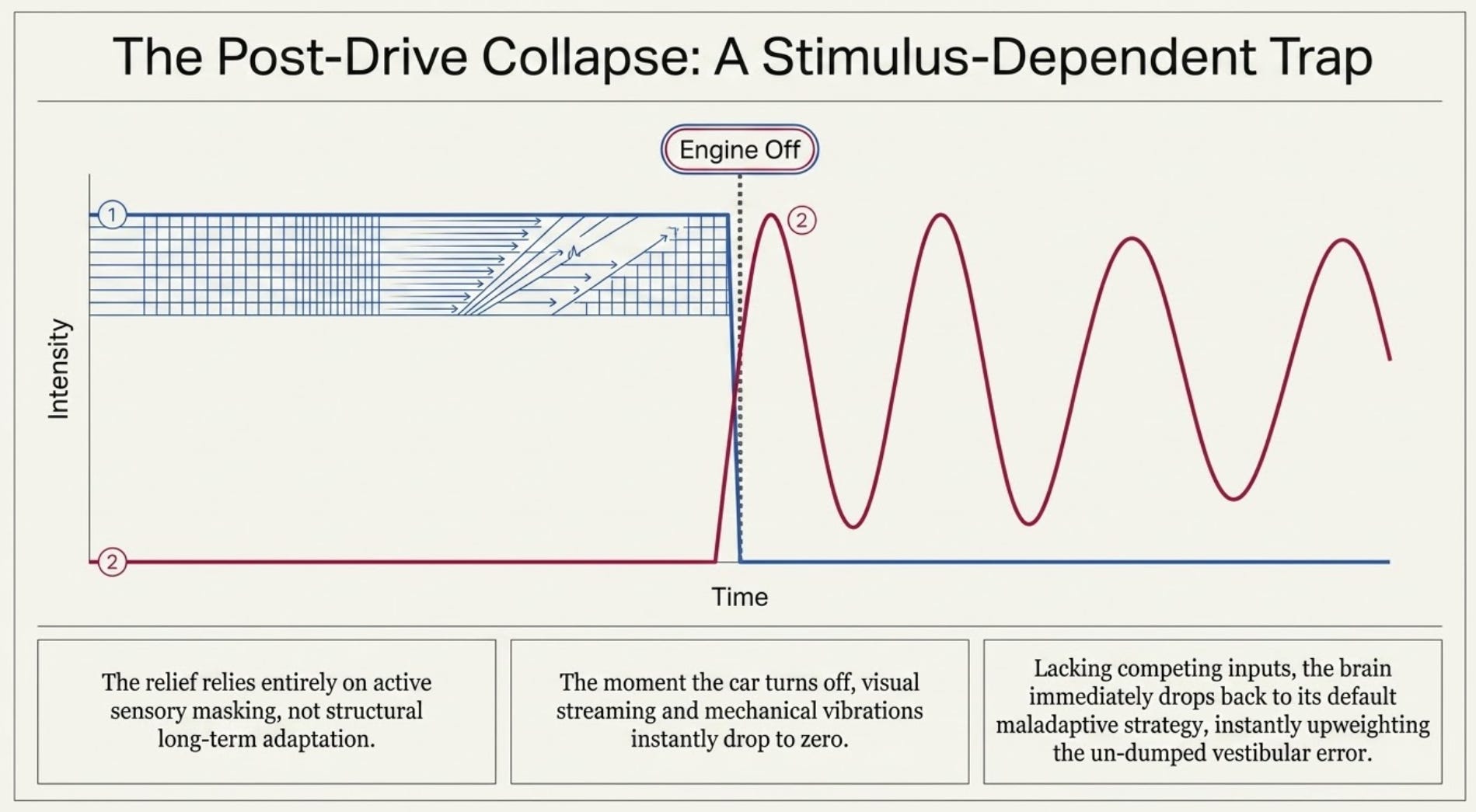
The moment the car turns off, the high-velocity visual streaming drops to zero, and the high-frequency somatosensory vibrations vanish. The patient is returned to a quiet, static environment. With no high-amplitude external signals left to mask the central nervous system, the brain immediately drops back to its default maladaptive sensory strategy (Tjernström et al., 2016).
Lacking any competing inputs, the central nervous system upweights the un-dumped, low-frequency internal vestibular reference, and the sensation of rocking or swaying reasserts itself instantly.
Conclusion
For the vestibular professional, analyzing the automobile effect through a sensory strategy lens provides a valuable diagnostic and therapeutic blueprint. It proves that the debilitating internal loop driving Mal de Debarquement Syndrome is not completely immutable; it can be pushed into the background when the central nervous system is forced to reweight its dependencies in response to congruent, high-amplitude external inputs. The ultimate challenge in vestibular rehabilitation is figuring out how to transition this temporary, stimulus-dependent masking into a long-term, long-lasting postural strategy.
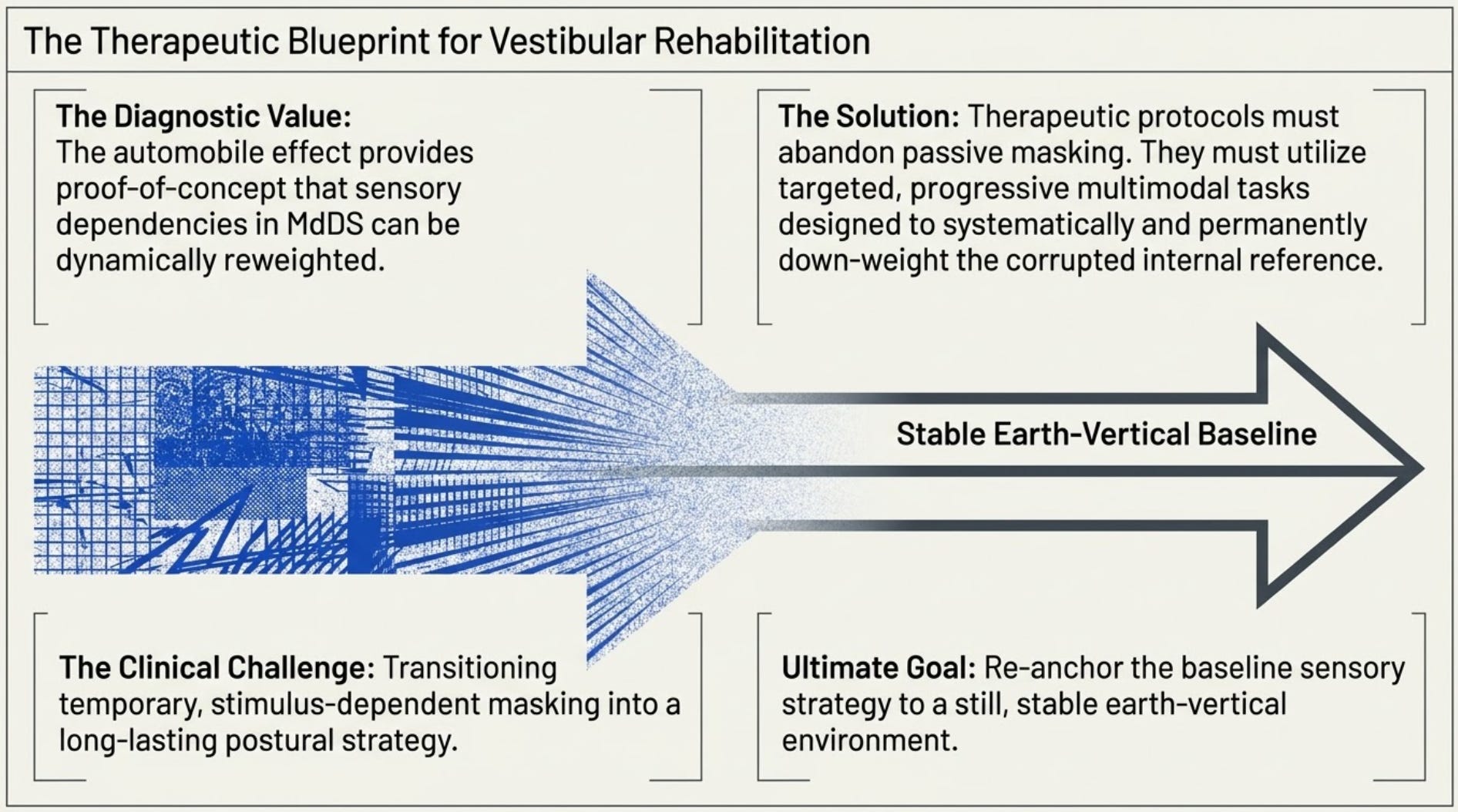
Rather than relying on transient external shunts, therapeutic protocols must utilize targeted, progressive multimodal tasks that systematically train the brain to permanently down-weight the corrupted internal vestibular reference and re-anchor its baseline sensory strategy to a still, stable earth-vertical environment.
Verifiable Clinical References
Barmack NH, Shojaku H. Vestibularly induced slow oscillations in climbing fiber responses of Purkinje cells in the cerebellar nodulus of the rabbit. Neuroscience. 1992;50(1):1-5. doi:10.1016/0306-4522(92)90376-d
Cohen B, Yakushin SB, Cho C. Hypothesis: The Vestibular and Cerebellar Basis of the Mal de Debarquement Syndrome. Frontiers in Neurology. 2018;9:28. doi:10.3389/fneur.2018.00028
Jeka J, Allison L, Kiemel T. Sensory reweighting dynamics in human postural control. Journal of Electromyography and Kinesiology. 2008;18(2):193-198. doi:10.1016/j.jelekin.2007.06.002
Peterka RJ. Sensorimotor integration in human postural control. Journal of Neurophysiology. 2002;88(3):1097-1118. doi:10.1152/jn.2002.88.3.1097
Tjernström F, Zur O, Jahn K. Current concepts and future approaches to vestibular rehabilitation. Journal of Neurology. 2016;263(Suppl 1):65-70. doi:10.1007/s00415-015-7962-6
In my experience with MdDS, I have found that the longer the drive, the more debilitating the unwinding. I always know not to make plans for activities when I arrive, give it a day or at least time to take a long nap if necessary. Thank you Brian.
This is intriguing stuff. I couldn't help but think about how it applies to astronauts both experientially and relative to treatment. With the absence of gravity as many as 80% of astronauts experience a related phenomenon called Space Adaptation Syndrome (SAS) or "terrestrial readaptation motion sickness". While Mal de Debarquement Syndrome (MdDS) is of course a specific terrestrial disorder (usually triggered by sea or air travel), astronauts face similar sensory-motor conflicts upon returning to gravity. For those prone to suffer from MdDS are there "pre-flight" exercises or routines that can be used to reduce the occurrence or severity of MdDS?