

The SINSS Model: A Framework for Clinical Reasoning in Concussion and Vestibular Care


For therapists specializing in vestibular and post-concussion management, the subjective examination is arguably the most critical component of the entire assessment. It is where we uncover the nuances of a patient’s experience, which guides a safe, effective, and targeted physical examination and treatment plan. The SINSS model, a powerful tool that organizes subjective information into five key domains, is not just effective in concussion care but also universally applicable to nearly any patient presentation. It helps us to be more empathetic and understanding, as we center our clinical reasoning on the unique experiences of each patient.
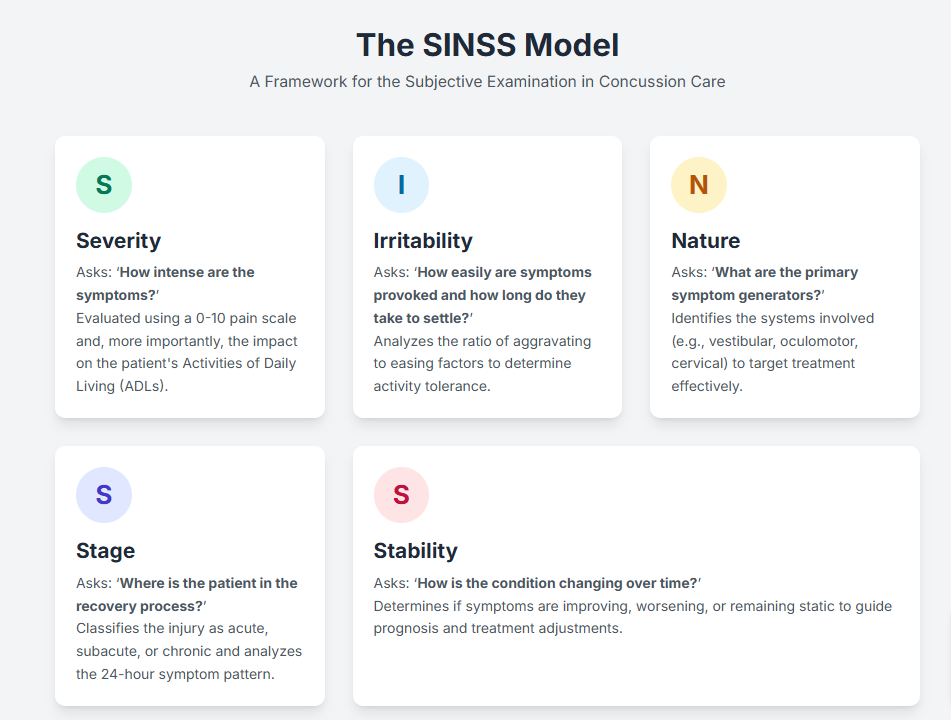
The SINSS model is an acronym that stands for Severity, Irritability, Nature, Stage, and Stability. By systematically exploring each of these areas, a therapist can build a comprehensive clinical picture that informs every subsequent decision.
Severity
Severity answers the fundamental question: ‘How intense are the patient’s symptoms?‘ This is assessed not only through a 0-10 numeric rating scale but, more critically, by its impact on the patient’s Activities of Daily Living (ADLs). A 3/10 headache that prevents a patient from tolerating screen time for work is far more severe functionally than a 7/10 headache that is present but does not limit their activity. Understanding severity helps establish the patient’s current functional baseline and is essential for goal setting and measuring progress.
Irritability
Irritability explores: ‘How easily are symptoms provoked, and how long do they take to resolve?‘ This is a crucial factor in determining the patient’s tolerance for physical assessment and therapeutic intervention. We analyze the ratio of aggravating factors to easing factors. A highly irritable condition is characterized by minimal activity triggering significant symptoms that take a long time to subside. Conversely, a low irritability condition requires a substantial amount of activity to provoke symptoms that resolve quickly. This insight directly informs the starting point and intensity of any intervention, ensuring we work within the patient’s tolerance to avoid symptom exacerbation.
Nature
The nature of the condition helps us hypothesize: ‘What are the primary symptom generators or underlying pathologies?‘ In the context of a concussion, this involves differentiating between potential drivers such as vestibulo-ocular dysfunction, cervical spine involvement, autonomic dysregulation, or physiologic post-concussion syndrome. The therapist acts as a detective, using the patient’s description of symptoms (e.g., spinning vertigo vs. lightheadedness; motion sensitivity vs. screen intolerance) to guide the subsequent objective testing and focus the treatment on the correct systems.
Stage
Stage addresses the timeline and progression of the condition, asking: ‘Where is the patient in the recovery process?‘ This involves classifying the injury as acute (days to weeks), subacute (weeks to months), or chronic (persisting for months or longer). The stage of healing significantly influences our prognosis, management strategies, and educational approach. We also examine the 24-hour pattern of symptoms. Are they worse in the morning, suggesting an inflammatory component? Do they build throughout the day with cognitive or physical load? This pattern provides clues about underlying mechanisms and informs recommendations for pacing and activity modification.
Stability
Finally, stability answers the question: ‘How is the condition changing over time?’ We need to determine if the patient’s overall symptom profile is improving, worsening, or remaining static. Is the patient making steady progress, or have they plateaued? A patient whose condition is deteriorating may signal a red flag or the need for a different management approach, whereas a stable or improving patient can be progressed more confidently. Assessing stability helps us understand the prognosis and make necessary adjustments to the plan of care.
By methodically applying the SINSS model, therapists can deconstruct a complex patient narrative into a clear, organized clinical profile. This structured approach elevates our clinical reasoning, ensuring that our treatment is not only evidence-based but also perfectly tailored to the individual sitting in front of us.
Brian K. Werner, PT, MPT, is a physical therapist who has been specializing in vestibular and balance disorders for over a quarter of a century. He is the founder of the FYZICAL Balance Paradigm and one of the co-founders of FYZICAL, LLC, Balance Center Division with Dr. Daniel Deems, MD, PhD, where he serves as the National Director of Vestibular Education & Training.