
The Standardization of Mediocrity: Why the Algorithm Failed the Patient


In vestibular rehabilitation, we often prioritize clinical consistency to reduce practice variation. However, the article ‘A Quality Improvement Project in Balance and Vestibular Rehabilitation and Its Effect on Clinical Outcome Measures’ by ALMohiza and colleagues reveals a striking disconnect. While therapist adherence to a ‘Clinical Treatment Algorithm (CTA)’ increased significantly, patient outcomes did not improve beyond those of patients receiving non-adherent care. To understand why, we must look at the foundation of their methodology: the framework established by Klatt et al. 2015, ‘A Conceptual Framework for the Progression of Balance Exercises in Persons with Balance and Vestibular Disorders.’
The Flaw of the Task-Based Framework
The algorithm used in this study relies heavily on a conceptual framework that emphasizes the ‘degree of difficulty’ and task progression. This approach assumes that simply making an exercise harder—moving from a stable to an unstable surface, or narrow to wide BOS—is the primary driver of recovery.
This methodology is fundamentally skewed because it prioritizes task completion over physiological resolution. For the specialized professional, a framework based solely on difficulty is clinically ineffective for several reasons:
Neglect of Sensory Mismatch: Effective vestibular therapy requires a precise focus on ‘sensory strategy’ and the specific mismatch causing the dysfunction. Simply increasing difficulty without addressing whether the patient is over-relying on visual or somatosensory cues does not promote true central compensation.
Ignoring Directionality: Vestibular deficits are often directional. A task-based progression often fails to target the specific plane of instability, resulting in generic exercises that do not resolve the underlying pathology.
Reinforcing Maladaptive Strategies: When we push a patient through a ladder of difficulty without correcting their ‘sensory strategy’, we risk reinforcing maladaptive compensations. The patient may ‘complete’ the harder task by utilizing an incorrect strategy, essentially cementing their dysfunction.
Analyzing the Statistical Failure
The statistics in the ALMohiza article confirm that adherence to a flawed model yields unremarkable results. While adherence improved by up to ‘12%’ (‘P = 0.008’), the clinical outcomes for the ‘ABC’ and ‘DHI’ showed no additional benefit from following the algorithm.
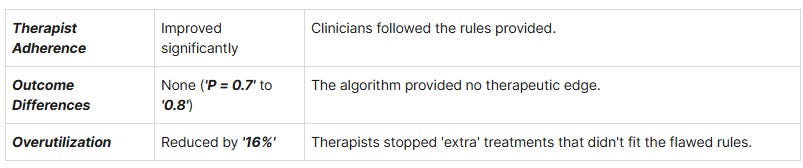
The study found that ‘balance activities’ were the most overutilized category. This suggests the algorithm’s narrow criteria likely labeled essential, nuanced sensory work as ‘unnecessary’ simply because it did not fit the generic task-based rules.
Conclusion: Beyond the Ladder of Difficulty
We must recognize that a ‘CTA’ is only as effective as the theory behind it. If we implement a framework that ignores ‘direction’ and ‘sensory mismatch’, we are merely standardizing a suboptimal process. High adherence to an ineffective algorithm is not a victory for quality improvement; it is the institutionalization of mediocrity.
As vestibular professionals, we should treat this study as a cautionary tale. We must build our protocols on the complexities of vestibular physiology—sensory weighting, directional specificity, and strategy correction—rather than a simplified ladder of task difficulty that fails to meet our patients’ needs.