
The Subcortical Mirror: Decoding the “Squishy Ground” and “Gravitational Pull” in MdDS


The mystery of Mal de Debarquement Syndrome (MdDS) often catches vestibular professionals off guard because it completely upends standard clinical logic.
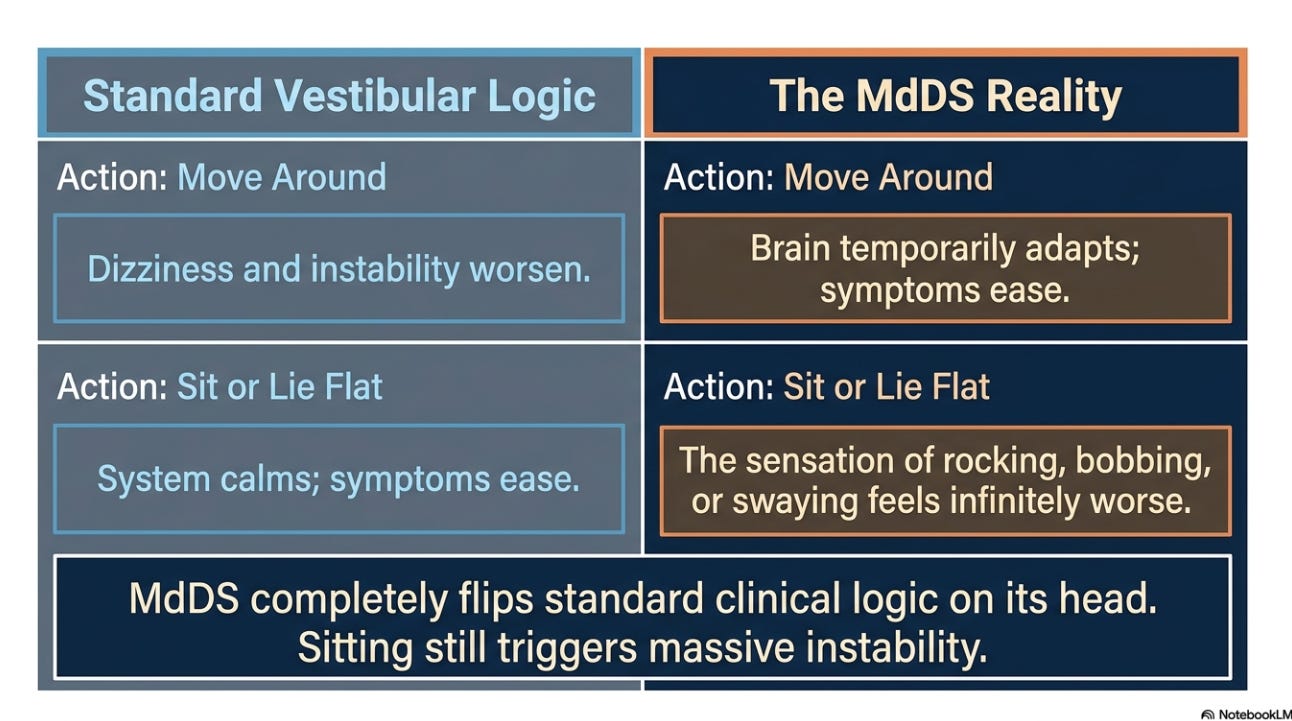
When a patient presents with classic vestibular symptoms, our standard advice is simple: if you feel dizzy or unstable, sit down and rest.
Yet, for an individual suffering from MdDS—whether it is classic motion-triggered or spontaneous (s-MdDS)—sitting at a desk or lying flat in bed can make the sensation of rocking, bobbing, or swaying feel infinitely worse.
To understand why this happens, we must look past the peripheral inner ear and peer directly into the subcortical spatial networks. By applying the clinical framework of Navigators vs. Stabilizers and examining the mechanics of the subcortical velocity-storage integrator, we can uncover exactly why the ground feels like a trampoline and why gravity feels like an invisible hand pulling the patient sideways.
The Squishy Ground: When the Silent Stabilizer Becomes a Noisy Navigator
In a healthy nervous system, upright postural control relies on a beautifully coordinated division of labor between two sensory processing modes:
The Stabilizers: These systems operate automatically in the background. Proprioception, somatosensory input from the soles of the feet, and baseline vestibular tone act as a silent anchor. They preserve your alignment against gravity without requiring conscious attention.
The Navigators: These systems—primarily active vision and dynamic vestibular tracking—engage when you actively move through, map, and interact with a changing environment.
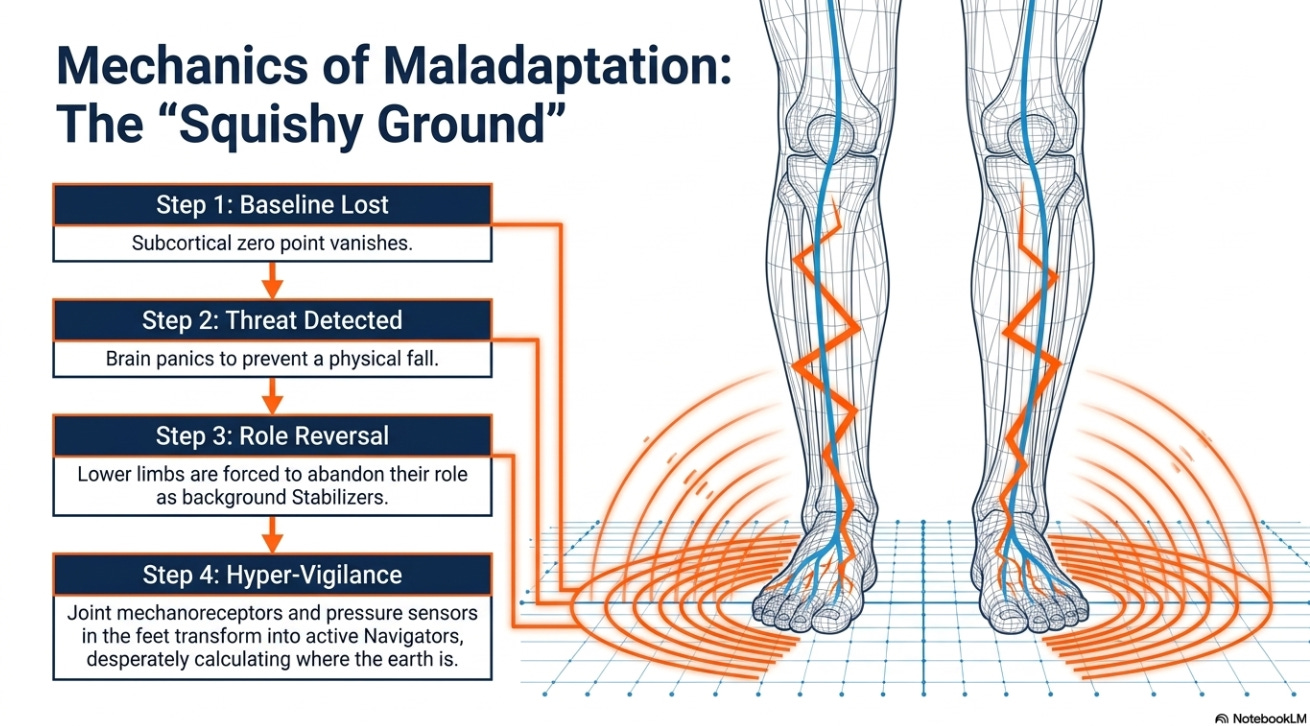
In an individual with MdDS, the internal subcortical baseline is completely disrupted. Because the central nervous system can no longer identify a true zero point, the silent subcortical anchor is lost.
To prevent a fall, the brain rapidly adopts a maladaptive sensory strategy. It forces the lower limbs and somatosensory pathways to shift roles, transforming them from a background Stabilizer into an active, high-alert Navigator.
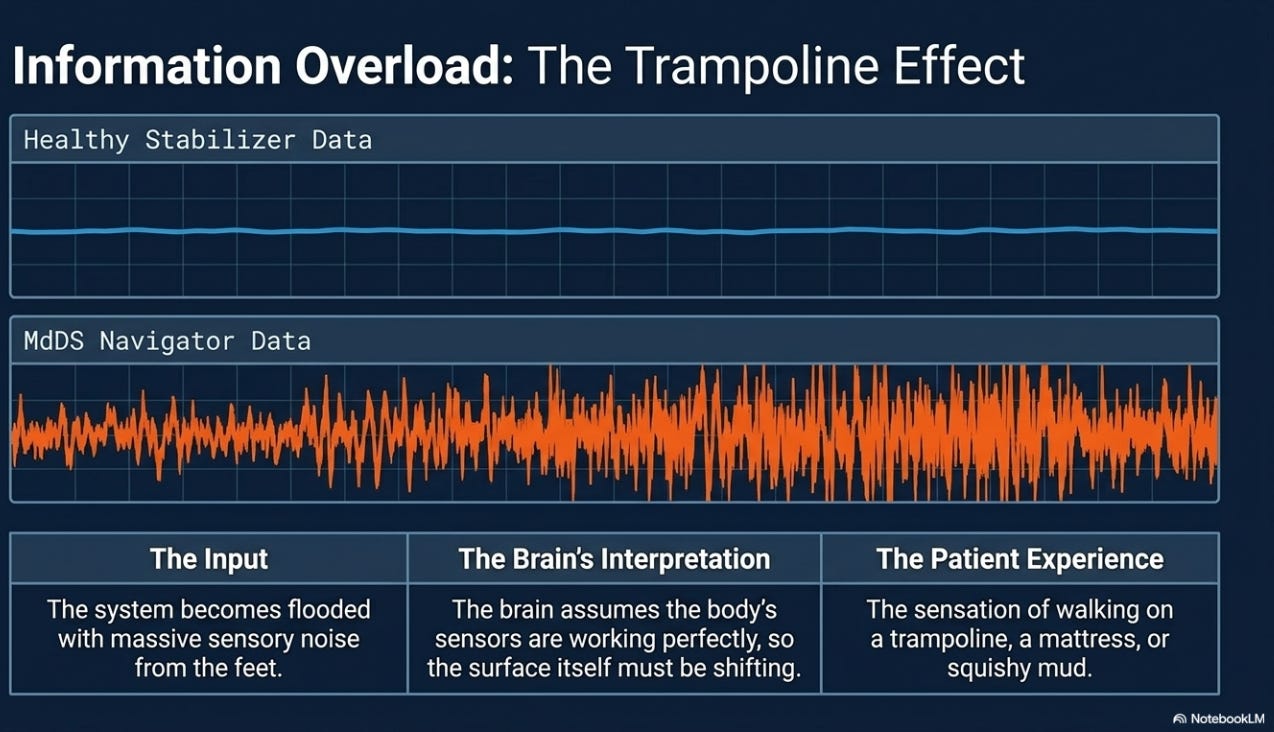
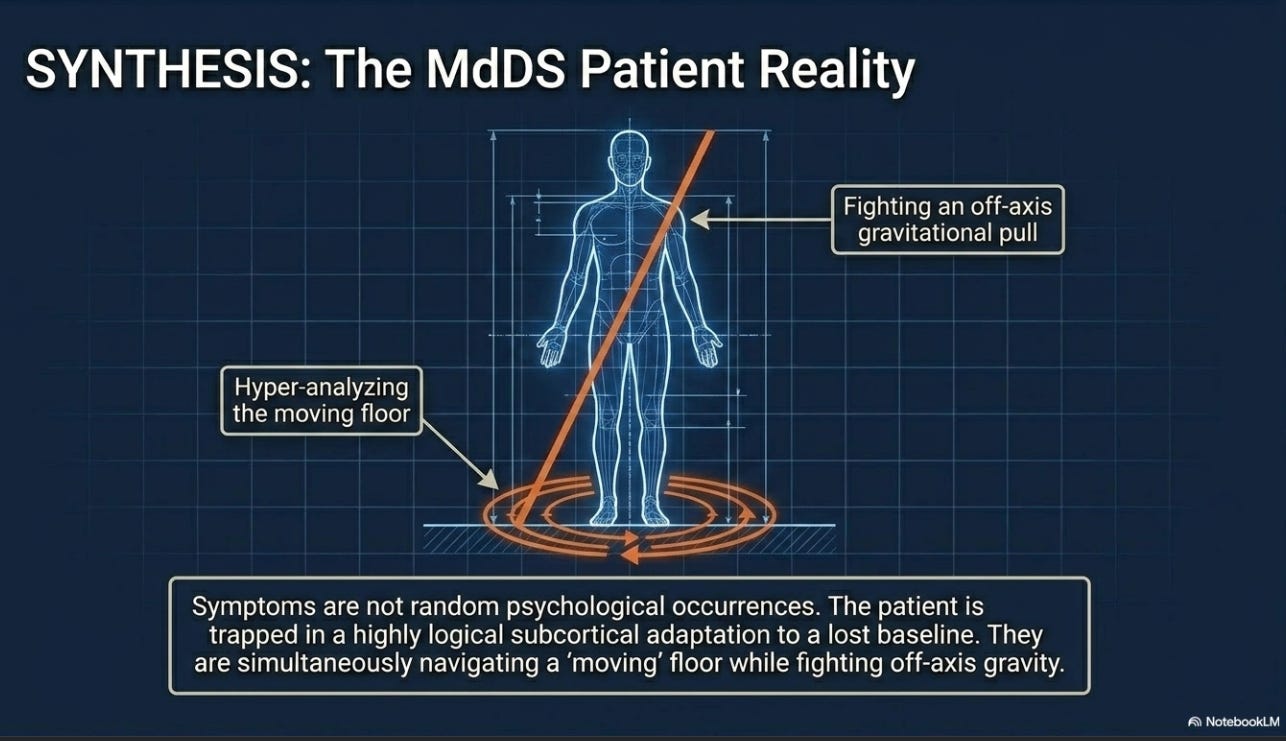
The patient begins hyper-analyzing every square inch of the floor, using joint mechanoreceptors and pressure sensors in the feet to actively calculate where the earth is. Because the lower limbs are now being used to aggressively navigate structural stability rather than silently stabilize posture, the system becomes flooded with noise. The brain interprets this massive, hyper-vigilant sensory influx as a shifting, unstable surface—causing the patient to feel as though they are walking on a trampoline, a mattress, or squishy mud.
Gravitational Pull: The Velocity Storage Integrator Out of Sync
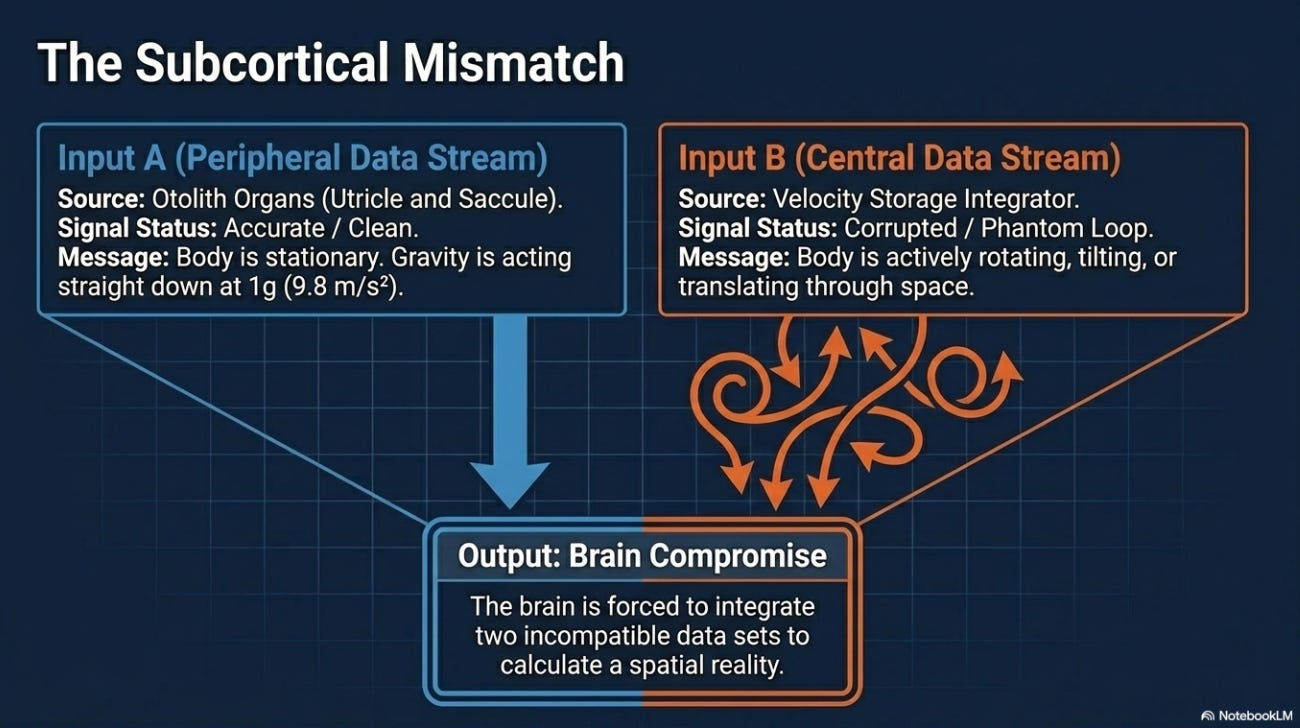
The second profound symptom frequently reported by these patients is a terrifying sensation of an unyielding gravitational pull—a feeling that they are being dragged heavily to one side or pulled downward into the floor. This spatial disorientation is a direct result of a subcortical mismatch involving the velocity storage integrator.
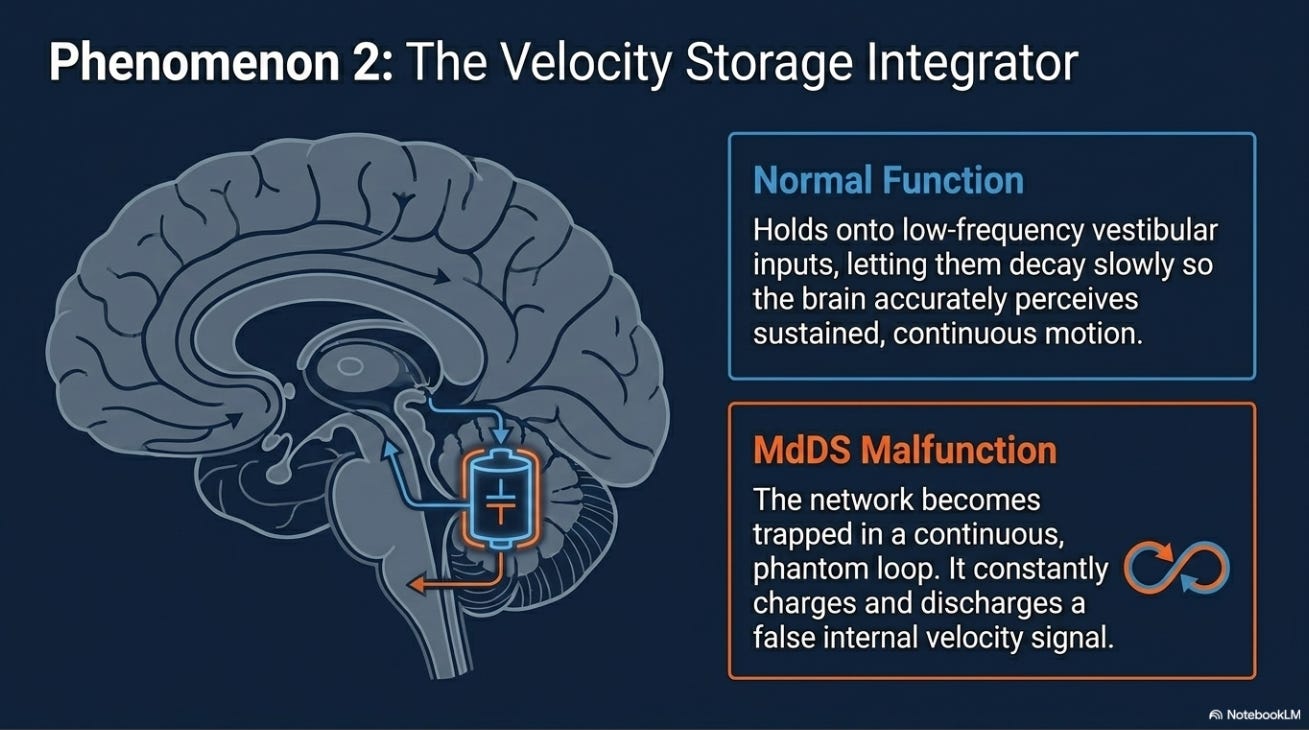
The velocity storage integrator is a specialized network of neurons located within the vestibular nuclei and the vestibulocerebellum (specifically the nodulus and uvula). It essentially functions as a storage tank for motion signals, holding onto low-frequency vestibular inputs and allowing them to decay slowly so the brain can accurately perceive sustained, continuous motion.
In MdDS, this velocity storage network becomes trapped in a continuous, phantom loop of motion, constantly charging and discharging an internal velocity signal. This creates an immediate subcortical conflict:
The Otolith Organs (Utricle and Saccule): These peripheral structures function perfectly. They send an accurate signal indicating that the body is stationary and that gravity acts straight downward at 1g (9.8 meters per second squared).
The Velocity Storage Integrator: This central network continuously broadcasts a corrupted signal insisting that the body is actively rotating, tilting, or translating through space.
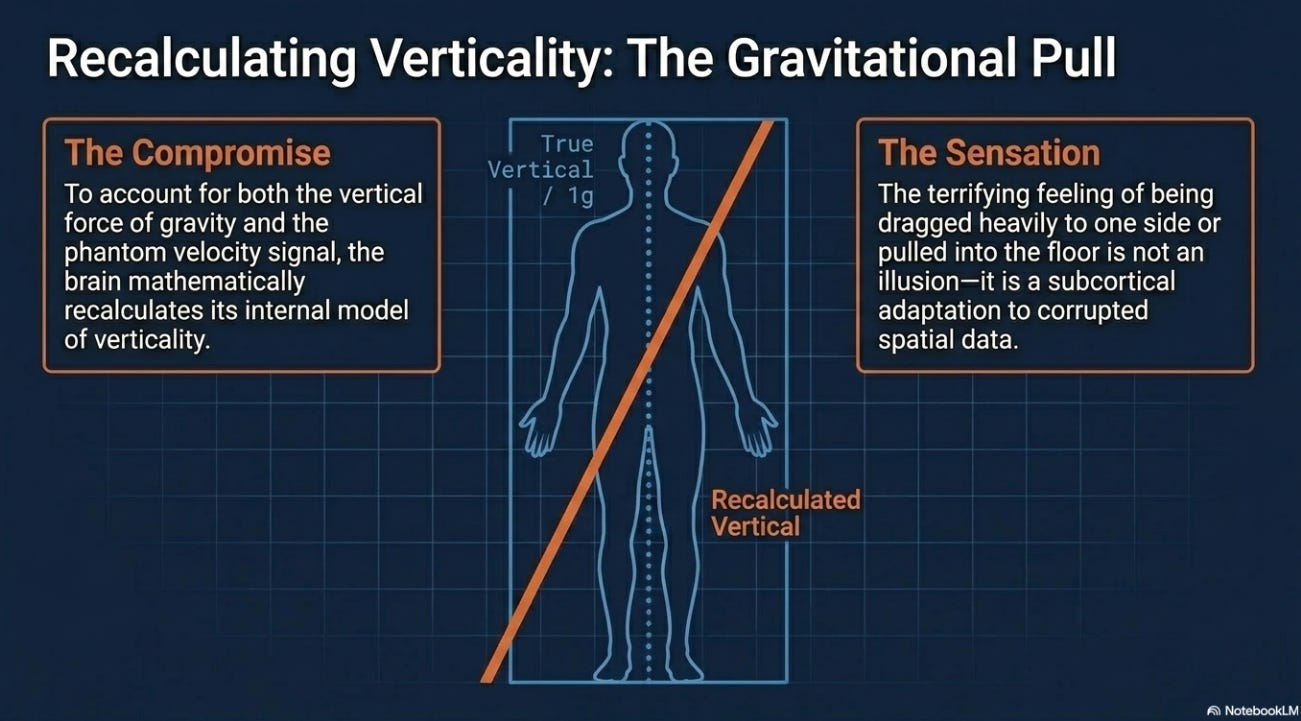
When the brain attempts to integrate these two incompatible data sets, it is forced to make a compromise. To account for both the vertical force of gravity and the phantom velocity signal, the brain recalculates its internal model of verticality. The resulting sensory mismatch convinces the patient that gravity is pulling them forcefully off-axis.
The Subcortical Blueprint for Rehabilitation
Ultimately, symptoms like the “squishy ground” and an artificial “gravitational pull” are not random occurrences; they are highly logical, subcortical adaptations to an internal vestibular baseline that has lost its zero point. When the brain cannot find its true vertical reference frame, it recruits the lower limbs to navigate stability and misinterprets gravity entirely.
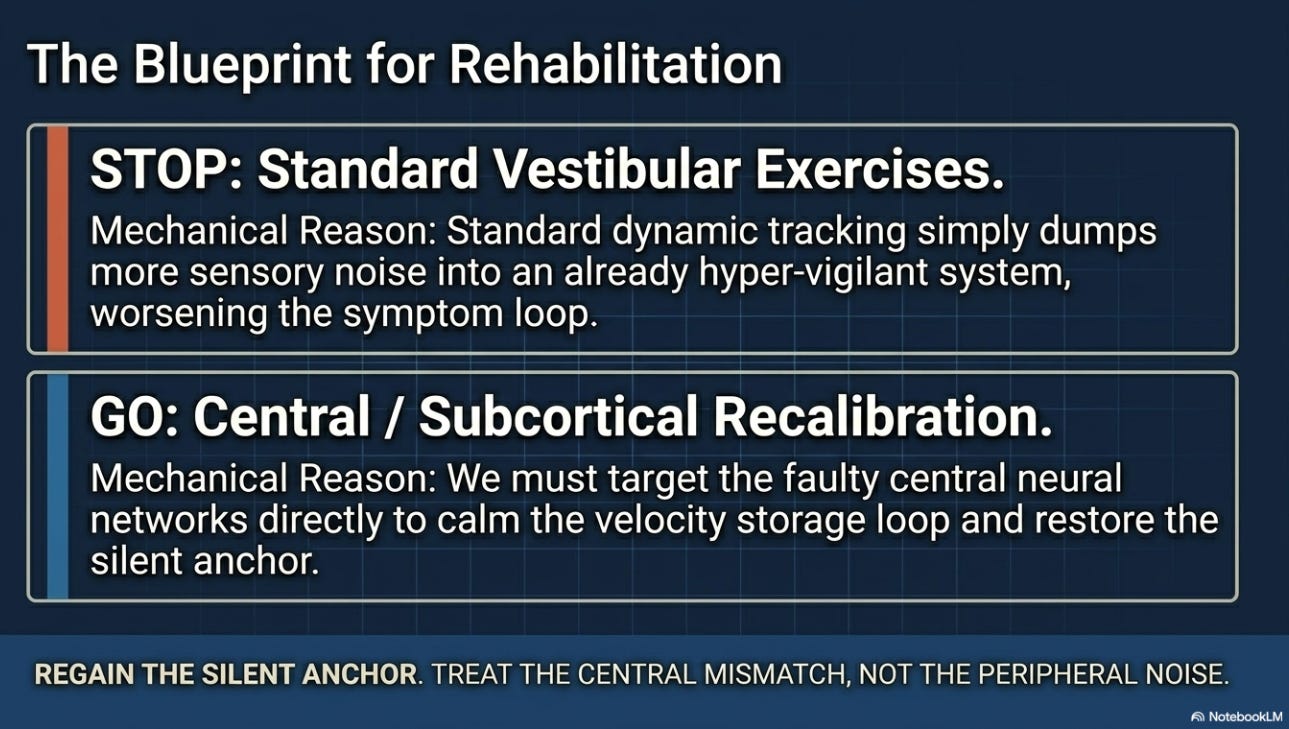
Recognizing this central sensory mismatch is the clinician's critical first step. We cannot treat this population effectively with standard vestibular exercises that simply introduce more noise. Instead, we must target the faulty neural networks directly to calm the system down and help the patient regain a silent, stable anchor.