


The Dix-Hallpike Maneuver
It's a ritual we know by heart, a dance we've performed countless times to diagnose Benign Paroxysmal Positional Vertigo (BPPV). We turn the patient's head, guide them swiftly back, and keenly observe the intricate ballet of nystagmus, those involuntary eye movements that whisper secrets of the inner ear. But sometimes, this familiar choreography takes an unexpected turn, a twist in the plot that challenges our assumptions and deepens our understanding of the vestibular system. Your role in this process is crucial, and your expertise is invaluable in deciphering these unexpected turns.
A Twist in the Tale: The "Wrong-Way" Nystagmus
Imagine a patient who presents with the classic complaints of episodic vertigo triggered by head movements. You confidently perform a Dix-Hallpike maneuver to the right, expecting the characteristic upbeat torsional nystagmus to the right, the hallmark of right posterior canal BPPV. But then, a surprise emerges – an upbeat torsional nystagmus to the left. A flicker of doubt might cross your mind. Is it a misinterpretation? An anatomical anomaly? Or a clue to a more profound mystery?
This "wrong-way" nystagmus, as counterintuitive as it seems, is not an anomaly but a gateway to a more nuanced understanding of the vestibular system. As seasoned professionals, it's a scenario we must be prepared for, a challenge that can refine our diagnostic acumen.
Unraveling the Paradox
While the Dix-Hallpike maneuver is designed primarily to assess the posterior canals, its reality is far more intricate. It can stimulate any of the three semicircular canals, adding layers of complexity to our diagnostic process.
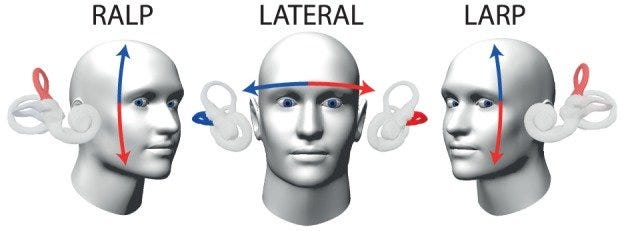
To decipher the "wrong-way" nystagmus, we must first delve into the functional pairing of the canals, known as the RALP (right anterior, left posterior) and LARP (left anterior, right posterior) planes. These planes dictate that the anterior canal on one side is functionally paired with the posterior canal on the opposite side, creating an intricate balance of excitation and inhibition.

Now, let's turn our attention to Ewald's Laws, which govern the relationship between endolymph flow (the fluid within the canals) and nystagmus:
Ewald's First Law states that each semicircular canal generates a unique eye movement pattern (ie, the slow phase or vestibular response) based on its anatomical position and neural connections to the ocular motor muscles. Thus, stimulating each canal will result in a specific and predictable nystagmus.
Ewald's Second Law applies specifically to horizontal canals. It states that ampullopetal flow (endolymph flow towards the ampulla) produces a more robust response than ampullofugal flow (flow away from the ampulla). This difference in response is due to the orientation of the hair cells within the crista ampullaris of the horizontal canal.
Ewald's Third Law governs the vertical canals (anterior and posterior). It states that ampullofugal flow is excitatory, while ampullopetal flow is inhibitory. This distinction from the horizontal canals is crucial for understanding the "wrong-way" nystagmus. It is also attributed to the orientation of the hair cells within the crista ampullaris of the vertical canals.
Armed with this knowledge, we can unravel the paradox:
Debris Movement: Otoconia dislodged from the utricle can travel through the common crus, the meeting point of the anterior and posterior canals.
Anterior Canal Inhibition: In this scenario, the otoconia enter the posterior arm of the right anterior canal. According to Ewald's Third Law, this causes ampullopetal endolymph flow (towards the ampulla), which inhibits the right anterior canal.
Unexpected Nystagmus: This inhibition of the right anterior canal leads to the observed upbeat torsional nystagmus to the left. Due to the RALP plane pairing, you are inhibiting the right anterior canal, which results in a relative excitation of the left posterior canal, producing the "wrong-way" nystagmus.
Why This Matters
This phenomenon underscores the need for a nuanced understanding of the vestibular system. It highlights our diagnostic challenges and the importance of accurate canal identification for effective treatment. Misinterpreting the nystagmus could lead to incorrect maneuvers and potentially worsen the patient's condition.
Beyond the Posterior and Anterior Canals
The Dix-Hallpike test can also stimulate the horizontal canals, leading to horizontal nystagmus (i.e., right-beating or left-beating). We must be vigilant in differentiating this from other causes of horizontal nystagmus to ensure an accurate diagnosis.
Dr. Asprella Libonati's Wisdom
Dr. Asprella Libonati's work on excitatory and inhibitory nystagmus provides a framework for understanding these complex scenarios. He emphasized the importance of "following the nystagmus" rather than relying solely on head position in diagnosing BPPV.

Treatment Strategies
When faced with the "wrong-way" nystagmus, consider the following:
Recognize Anterior Canal Involvement: The most likely cause is debris in the posterior arm of the right anterior canal.
Modified Maneuvers: To address anterior canal BPPV, employ a modified maneuver, such as a variation of the Yacovino maneuver. Bring the patient directly to a sitting position.
Observe Orthotropic Nystagmus: When the patient sits up, observe for orthotropic nystagmus, which should be a rightward, downbeat torsional nystagmus, confirming excitation of the right anterior canal.
Conclusion
The unexpected Dix-Hallpike reminds us that BPPV assessment requires more than a superficial understanding. By recognizing the potential for unexpected canal activation, incorporating knowledge of RALP/LARP planes and Ewald's Laws, and meticulously interpreting nystagmus patterns, we can improve diagnostic accuracy and deliver superior patient care. This awareness keeps us alert and prepared for any twist in the plot.
Let's continue to challenge our assumptions, refine our diagnostic skills, and embrace the vestibular system's complexities. Only then can we truly master the art of BPPV diagnosis and management. This journey of understanding and mastering the vestibular system's complexities should motivate and engage us in our professional development.