
The Universal Repositioning Maneuver: A Paradigm Shift in BPPV Management - with Potential for Safer Home Treatment


Benign paroxysmal positional vertigo (BPPV) is a cornerstone of vestibular rehabilitation, yet its management remains nuanced even for seasoned practitioners. While effective, the current array of canalith repositioning maneuvers (CRMs) demands precise diagnosis and execution, particularly in atypical or multicanal presentations.
The Complexity of BPPV in Vestibular Practice
BPPV's protean clinical manifestations, encompassing diverse nystagmus patterns and symptom severity, can challenge even the most experienced vestibular therapists. Multicanal BPPV, in particular, often necessitates prolonged treatment plans with multiple CRMs, increasing patient burden and potentially impacting adherence. Patients with complex medical histories or physical limitations may also require tailored treatment approaches, further complicating clinical decision-making.
Unveiling the Universal Repositioning Maneuver (URM)
The Universal Repositioning Maneuver (URM) emerges as a potential breakthrough theoretically capable of treating BPPV irrespective of the affected canal, including multicanal cases. This novel maneuver has undergone rigorous testing using a 3D biomechanical model of the human labyrinth. It demonstrates its potential to effectively reposition otoliths from all three semicircular canals back to the utricle.
Potential for Safer Home Treatment
The URM's relative simplicity and adaptability offer a safer home treatment alternative than more specific CRMs. Its reduced complexity and lower risk of provoking severe vertigo or complications could empower patients to manage their BPPV symptoms under appropriate guidance.
However, it's crucial to emphasize that proper instruction and supervision by a qualified healthcare professional are paramount before attempting home treatment.
How to Perform the URM
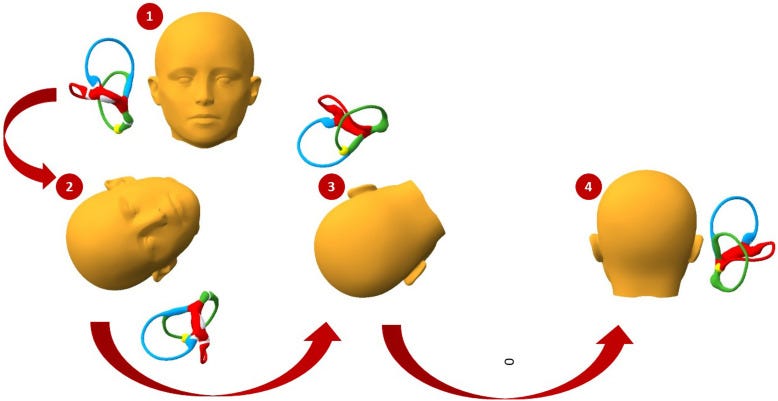
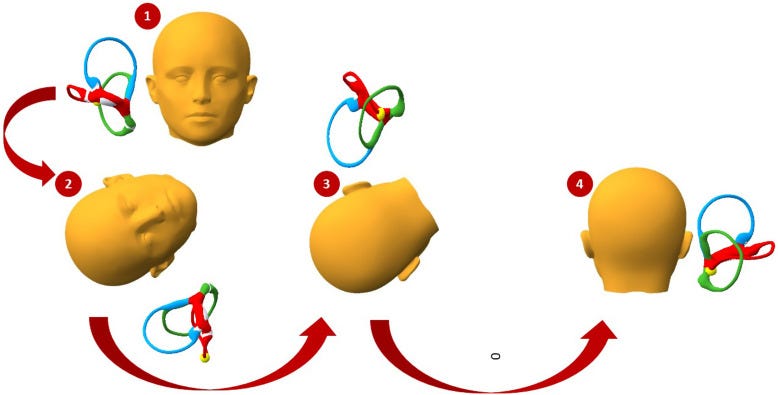
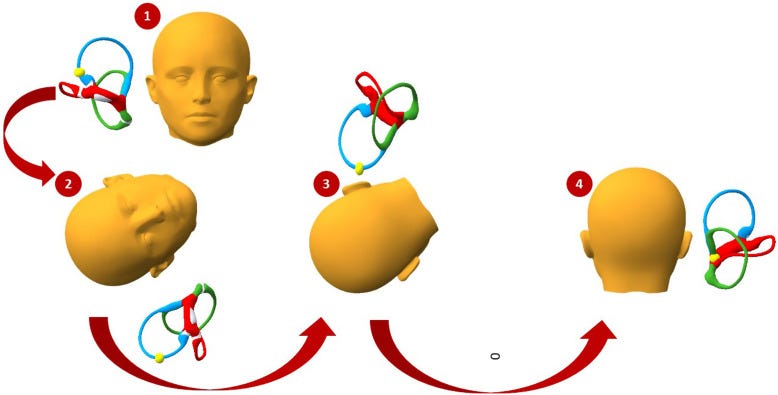
The URM consists of four sequential steps:
Starting Position: The patient is seated upright on the edge of a treatment table or firm surface, with their legs hanging down and head in a neutral position (facing forward).
Lie Down on Affected Side: The patient gently lies down on the side of their affected ear, ensuring their head remains tilted slightly upward at an angle of approximately 30-45 degrees. If necessary, a pillow can be placed under the shoulder to facilitate this head position.
Note: The recommended hold time is 1 minute once symptoms have stopped.
Roll onto the Opposite Side: Maintaining the same head tilt, the patient slowly rolls their body 180 degrees onto the unaffected side. The therapist may assist in guiding this movement to ensure a smooth transition.
Note: the recommended hold time is 2 minutes once symptoms have stopped.
Sit Up: The patient slowly returns to an upright seated position, keeping their head in a neutral position throughout.
How the URM Addresses Each Canal
The URM's sequential head and body movements create a unique pathway for otolith repositioning, effectively targeting each of the three semicircular canals:
Posterior Canal:
The initial side-lying position with the affected ear down utilizes gravity to encourage otolith movement out of the posterior canal.
The subsequent roll to the opposite side further facilitates otolith migration towards the common crus and, ultimately, the utricle.

HSC - BPPV - APO
HSC-BPPV - GEO
Lateral Canal:
The head tilt during the side-lying positions helps to dislodge otoliths from the lateral canal's ampullary and non-ampullary arms.
The 180-degree roll reorients the canal, allowing gravity to move the otoliths towards the utricle.
Anterior Canal:
Although less commonly affected, the URM's head positions and body roll create a pathway for otoliths to move out of the anterior canal and into the utricle.
Clinical Implications for Vestibular Therapists
The URM has the potential to revolutionize BPPV management in several key ways:
Diagnostic Efficiency: The URM simplifies clinical decision-making, reducing reliance on intricate diagnostic procedures and potentially expediting treatment initiation.
Accelerated Recovery: The potential for faster symptom resolution, especially in multichannel BPPV, optimizes patient outcomes and resource utilization, allowing therapists to manage a larger caseload effectively.
Enhanced Patient Experience: The URM's adaptability accommodates patients with diverse needs, including those with physical limitations or comorbidities, potentially improving adherence and satisfaction.
Expanded Treatment Horizons: The URM's versatility may facilitate BPPV management in various settings, including home programs and telehealth, broadening access to care and empowering patients to participate actively in their recovery.
Safer Home Treatment Option: The URM's relative simplicity and lower risk profile than other CRMs may make it a suitable candidate for home treatment under appropriate guidance and supervision.
Looking Ahead & Call to Action
While the URM shows immense promise, clinical trials are essential to validate its effectiveness and safety in clinical and home settings. We urge vestibular therapists to stay abreast of ongoing research and consider participating in future studies evaluating the URM's clinical utility.
By integrating the URM into our clinical armamentarium, we have the potential to revolutionize BPPV management, elevate patient care to new heights, and solidify our role as leaders in vestibular rehabilitation.
Key Points to Emphasize:
The URM can potentially streamline BPPV management, particularly for complex cases.
Provide a clear explanation of how to perform the URM, including the positioning and movements involved.
The potential of the URM as a safer home treatment option under appropriate guidance.
Clinical trials are essential for validating their effectiveness and safety.
The URM's potential to enhance patient outcomes and expand treatment accessibility.
There is a need for continued research and professional development in BPPV management.
Let us embrace this exciting development and explore its possibilities for transforming the landscape of BPPV treatment.
References:
Barreto RG, Yacovino DA, Cherchi M, Teixeira LJ, Nader SN, Leão GF. Universal Repositioning Maneuver: A New Treatment for Single Canal and Multi-Canal Benign Paroxysmal Positional Vertigo by 3-Dimensional Model Analysis. J Int Adv Otol. 2023 Jun;19(3):242-247. doi: 10.5152/iao.2023.22921. PMID: 37272643; PMCID: PMC10331719.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10331719/
Disclaimer:
The information presented in this article is for educational purposes only and should not be construed as medical advice. Always consult a qualified healthcare professional regarding health conditions before making treatment decisions.