
The Vestibular Paradox in the Use of Benzodiazepines: A Substack Article for Professionals and Patients


Disclaimer: I am a physical therapist and writer, not a medical doctor. The information in this article is based on a synthesis of existing research and is for educational purposes only. It is not intended as medical advice. You should always consult with your physician or a qualified healthcare professional before making any decisions about your treatment or medications, particularly when it comes to benzodiazepines.
For those who live with vestibular disorders, the world can feel like a constantly moving ship on a stormy sea. The sense of imbalance, the overwhelming dizziness, and the accompanying panic can be profoundly debilitating. In a vestibular crisis, a medication that can calm the storm seems like a lifeline. Benzodiazepines, a class of drugs with powerful sedative and anxiolytic properties, often fill that role. Yet, their use in vestibular care presents a fundamental paradox: the very tool that offers immediate relief can, in the long run, actively hinder the brain's ability to recover.
The article, written for both vestibular professionals and patients facing the challenge of vestibular dysfunction, will delve into this crucial topic.
For the Vestibular Professional: Navigating the Neurobiological and Clinical Contradiction
The cornerstone of long-term recovery from a vestibular insult is central vestibular compensation—a dynamic process of neuroplasticity that rebalances the central nervous system to restore equilibrium. Vestibular rehabilitation therapy (VRT) is designed to facilitate and accelerate this process.
Vestibular compensation occurs through four primary neuroplastic mechanisms:
Adaptation: The brain adjusts the gain and phase of its reflexive responses to match the new reality of the lesioned labyrinth. Adaptation is not limited to a single reflex; it is a profound process that applies to all vestibular reflexes, including the vestibulo-ocular reflex (VOR), which stabilizes visual gaze, the vestibulo-colic reflex (VCR), which stabilizes the head and neck, and the vestibulo-spinal reflex (VSR), which generates compensatory body movements to maintain balance and posture. The cerebellum mainly controls the ability to adapt and fine-tune motor programs.
Substitution: Sensory substitution is an ongoing process that occurs throughout central compensation. The central nervous system uses other sensory systems to compensate for vestibular input that is not working correctly, relying more heavily on visual cues and proprioceptive inputs from the body to maintain balance and orientation.
Habituation and Desensitization: These related but distinct processes enable the brain to reduce its response to a stimulus that provokes it. Habituation is a form of non-associative learning where the brain passively learns to ignore or suppress an abnormal signal over time. In contrast, desensitization therapies are a more active and behavioral approach that aims to decrease the brain's sensitivity to triggers through deliberate and repeated exposure to provocative movements or stimuli. Both processes are crucial for reducing dizziness and helping the brain get used to sensations that once caused vertigo.
A delicate balance of excitatory and inhibitory signals in key brain regions, such as the vestibular nuclei and the cerebellum, tightly regulates these complex adaptive processes. The principal inhibitory neurotransmitter in the brain is gamma-aminobutyric acid (GABA). If the nervous system were a car, GABA is the 'brakes'. Benzodiazepines, such as diazepam (Valium) and lorazepam (Ativan), work by binding to the GABA-A receptor and acting as a 'booster', which dramatically enhances GABA's inhibitory action.
By powerfully suppressing neuronal excitability, benzodiazepines reduce the aberrant signals that cause vertigo. Researchers have demonstrated the direct depressant action of these drugs at the lateral vestibular nucleus, a central hub for processing vestibular information. This is why they effectively quiet the system in an acute crisis.
However, the very mechanism that provides short-term relief makes prolonged benzodiazepine use counterproductive to long-term recovery. By applying a global pharmacological brake to the nervous system, benzodiazepines interfere with the very synaptic plasticity and neural re-wiring required for compensation to occur. The interference with synaptic plasticity is not merely a theoretical concern; a substantial body of evidence and clinical guidelines support this conclusion. For instance, a systematic review and meta-analysis concluded that single-dose antihistamines provided greater vertigo relief at two hours than single-dose benzodiazepines, and long-term daily benzodiazepine use was not associated with improved outcomes for acute vertigo. Furthermore, professional organizations, such as the American Academy of Otolaryngology-Head and Neck Surgery, explicitly recommend against the routine use of vestibular suppressants for benign paroxysmal positional vertigo (BPPV), as canalith repositioning procedures are the first-line, evidence-based treatment.

For the Patient: Understanding the Pros and Cons
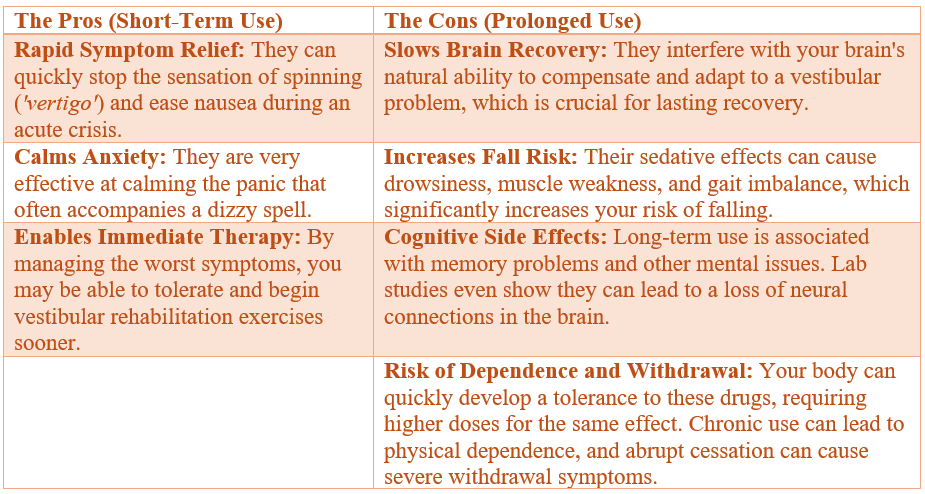
Experiencing a sudden, severe vertigo attack can be one of the most frightening things a person can go through. The feeling of the world spinning uncontrollably, coupled with intense nausea and a loss of balance, can trigger profound anxiety and panic. Benzodiazepines offer a powerful and much-needed escape from immediate distress. They can quickly calm the vertigo and the panic that comes with it, providing you with a 'rescue' medication for a severe episode. Doctors often use them for the first 1-3 days of a vestibular crisis to manage overwhelming symptoms.
However, if you've been on these medications for an extended period, you must understand why they are not a long-term solution.
The Pros (Short-Term Use) The Cons (Prolonged Use) - Stop and Review the Table
A Special Note on Anxiety: The relationship between vestibular symptoms and anxiety is a two-way street. A vestibular problem can trigger anxiety, and anxiety can, in turn, make your vestibular symptoms feel worse. The interaction creates a vicious cycle. If you have a diagnosed anxiety disorder (as per DSM-5 criteria), you must manage it. However, a purely pharmacological approach to both conditions is often ineffective in the long term. The most successful treatment is a multi-disciplinary approach that combines VRT, which restores your physical stability, with psychological and behavioral support, such as Cognitive Behavioral Therapy (CBT). This holistic model improves both physical and mental health, helping you regain confidence and functionality.
Conclusion
The evidence is clear: benzodiazepines are a temporary bridge, not a destination. They have a valuable, albeit limited, role as a 'rescue' medication for the initial days of a severe vestibular crisis, providing relief while you work with your healthcare team to develop a long-term plan. The true path to lasting recovery lies in the brain's own capacity to heal and adapt through vestibular rehabilitation.
You must work with a knowledgeable vestibular professional to get off these medications safely and begin the active process of rehabilitation.
Final Disclaimer: The information presented here is for educational purposes only. I am a physical therapist with 26 years of experience in the field of vestibular therapy, not a medical doctor. I do not recommend that anyone come off these medications without speaking to their medical doctor. Please consult with your physician or a qualified healthcare professional before making any changes to your medication regimen. My purpose in writing this article is to inform both professionals and patients about the paradox of benzodiazepine use in vestibular care. As a physical therapist, my role is to provide education and therapeutic interventions for balance disorders, rather than managing or prescribing medications.
References
roMotion Rehab & Sports Medicine. (2024, March 29). A Key To Vestibular Rehab: Habituation. Retrieved from https://physiosc.com/media/a-key-to-vestibular-rehab-habituation-
Sharif, S., Edlow, J. A., et al. (2023). Vestibular suppressants for benign paroxysmal positional vertigo: A systematic review and meta-analysis of randomized controlled trials. Academic Emergency Medicine, 30(5), 541-551.
Neurophysiology of Vestibular Compensation. (2023, January). Audiology and Speech Research, 19(1), 1-16.
The Role of GABAB Receptors in the Auditory System. (2023). Frontiers in Endocrinology. https://doi.org/10.3389/fendo.2023.1195038