
Understanding Bilateral Vestibular Weakness (BVW): Diagnostic Mastery And Emerging Therapeutics


Bilateral vestibular weakness (BVW) is a pathological reduction of vestibular signals from one or more labyrinthine inputs on each side due to lesions of the end organelles, their afferent pathways, or a combination of both. This physiological state results in severe functional disability, presenting primarily as a combination of oscillopsia and chronic postural unsteadiness. Diagnostic confirmation requires instrumented vestibular testing demonstrating impaired or absent function of the vestibulo-ocular reflex (VOR) across specific frequency ranges.
The foundational source for this discussion is the open-access review article, “Bilateral Vestibular Weakness and its Management,” by Marcello Cherchi, published on March 23, 2026, in the medical journal Current Treatment Options in Neurology (Volume 28, Article Number 5).
What Are The Current Diagnostic Criteria For Bilateral Vestibular Weakness?
Clinical suspicion begins at the bedside, but formal diagnosis requires objective quantification.
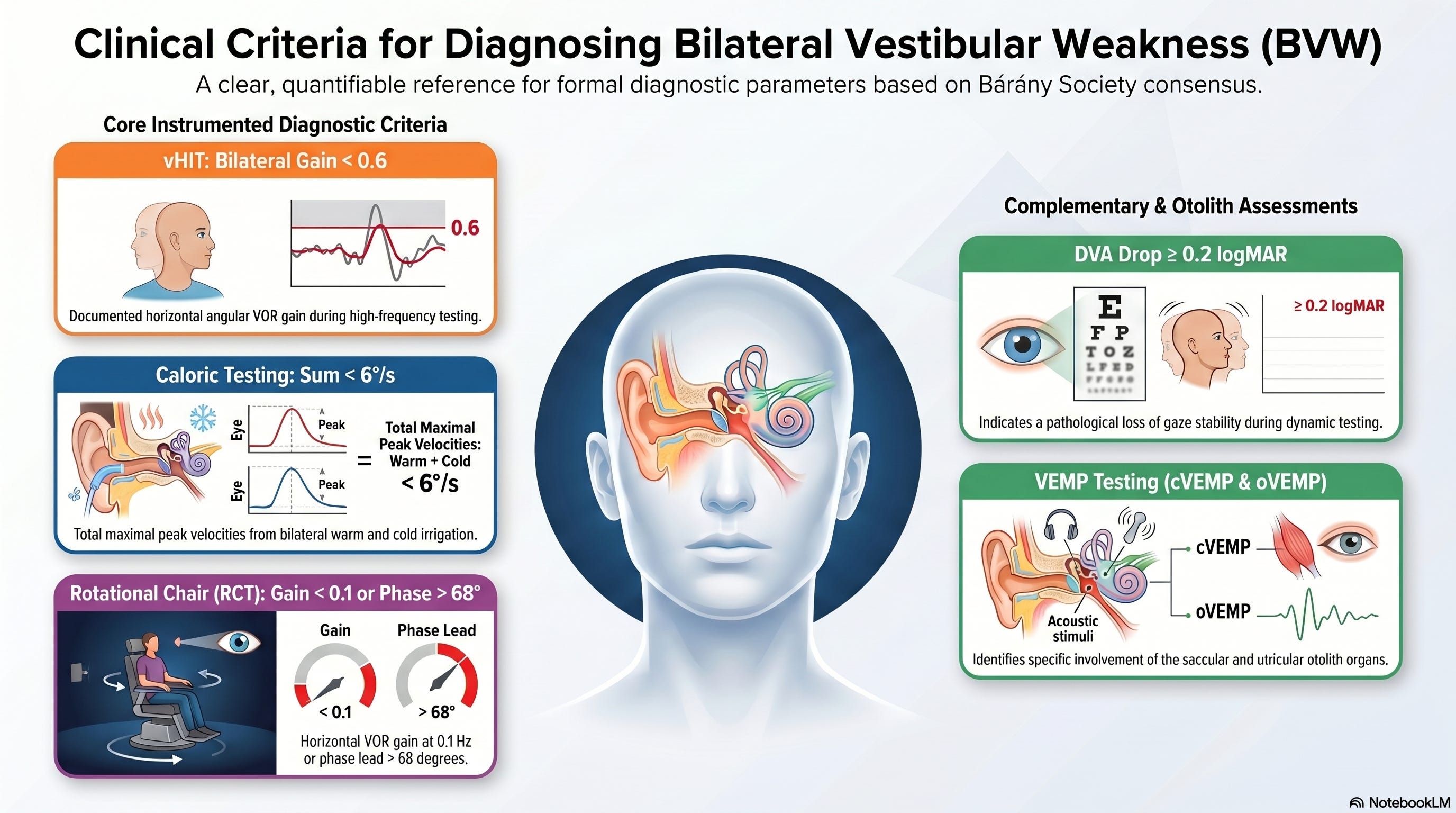
“The Bárány Society consensus criteria define BVW through specific instrumented parameters.”
The diagnostic criteria and testing parameters for vestibular dysfunction become much more accessible when broken down into distinct, scannable clinical benchmarks.
Here is the rewritten version, organized by testing modality for improved clarity:
Primary Diagnostic Criteria
Video Head Impulse Testing (vHIT) or Scleral Coil Technique (High-Frequency Assessment)
Requires a documented horizontal angular vestibulo-ocular reflex (VOR) gain of < 0.6 on both sides.
Caloric Testing (Low-Frequency Assessment)
Must demonstrate that the sum of the maximal peak velocities of the slow-phase, caloric-induced nystagmus from bilateral warm and cold irrigation is < 6°/s.
Rotational Chair Testing (RCT) (Mid-to-Low Frequency Gold Standard)
Must show a horizontal angular VOR gain of < 0.1 at 0.1 Hz, or a phase lead greater than 68 degrees (which is equivalent to a time constant of < 5 seconds).
Complementary Diagnostic Testing
Dynamic Visual Acuity (DVA)
A drop of ≥ 0.2 logMAR indicates a pathological loss of gaze stability.
Vestibular-Evoked Myogenic Potentials (cVEMPs and oVEMPs)
These tests are not embedded in the formal diagnostic definition, but they serve a vital role in identifying specific otolith (saccular and utricular) involvement.
Why Do Semicircular Canal Deficits Vary Across The Vestibular Tuning Spectrum?
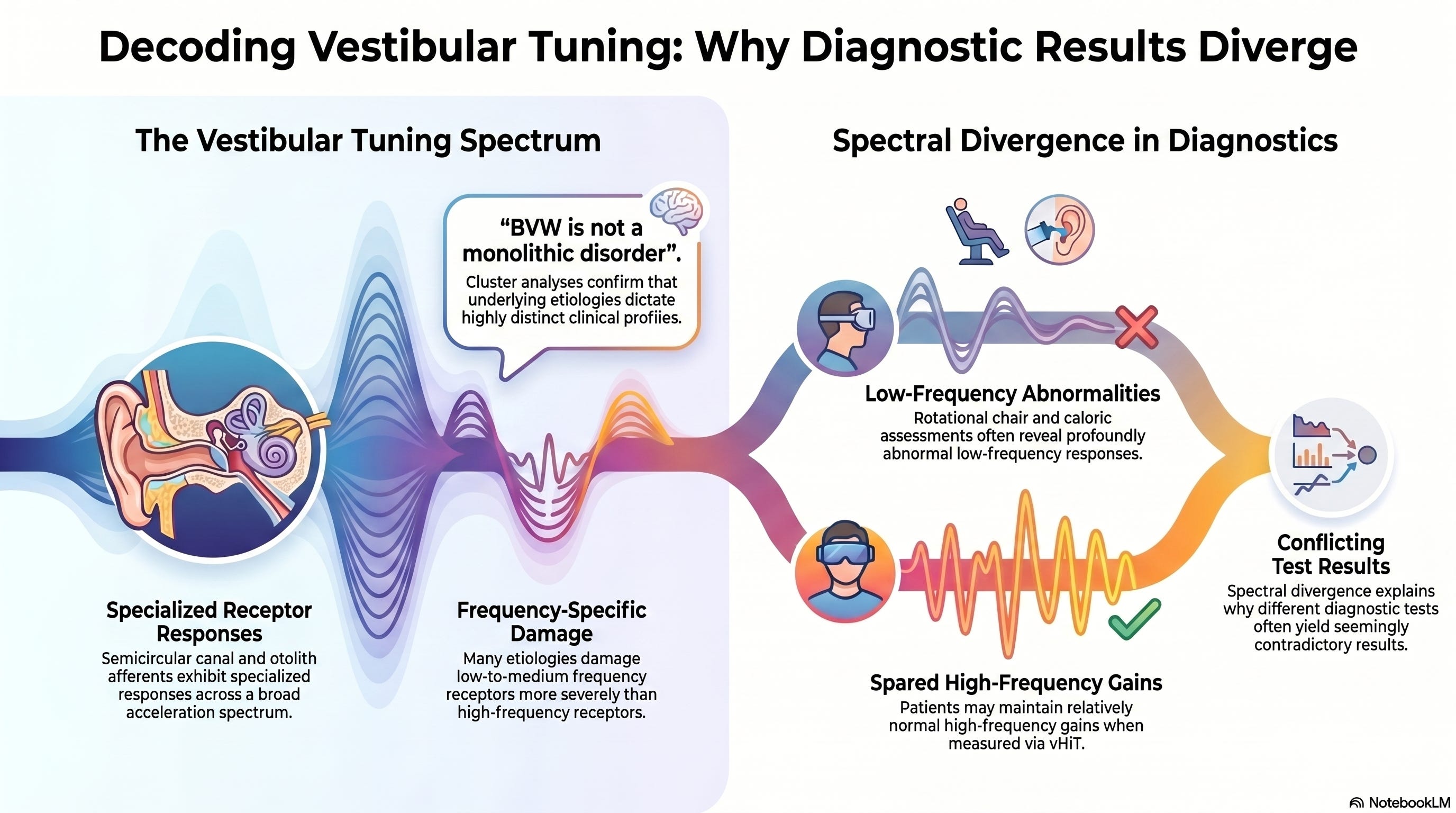
Semicircular canal and otolith afferents exhibit highly specialized responses across a broad acceleration spectrum.
The human medical literature rarely addresses this “vestibular tuning spectrum,” yet it helps explain why diagnostic test results often conflict. Many etiologies of BVW damage low- to medium-frequency receptors more severely than high-frequency receptors.
Consequently, a patient may demonstrate profoundly abnormal low-frequency responses on a rotational chair or caloric assessment, while maintaining relatively spared high-frequency gains on vHIT.
“This spectral divergence highlights why BVW is not a monolithic disorder.”
Hierarchical cluster analyses confirm that underlying etiologies dictate highly distinct clinical profiles and specific patterns of labyrinthine destruction.
How Should Clinicians Segment Idiopathic Versus Genetically Driven BVW?
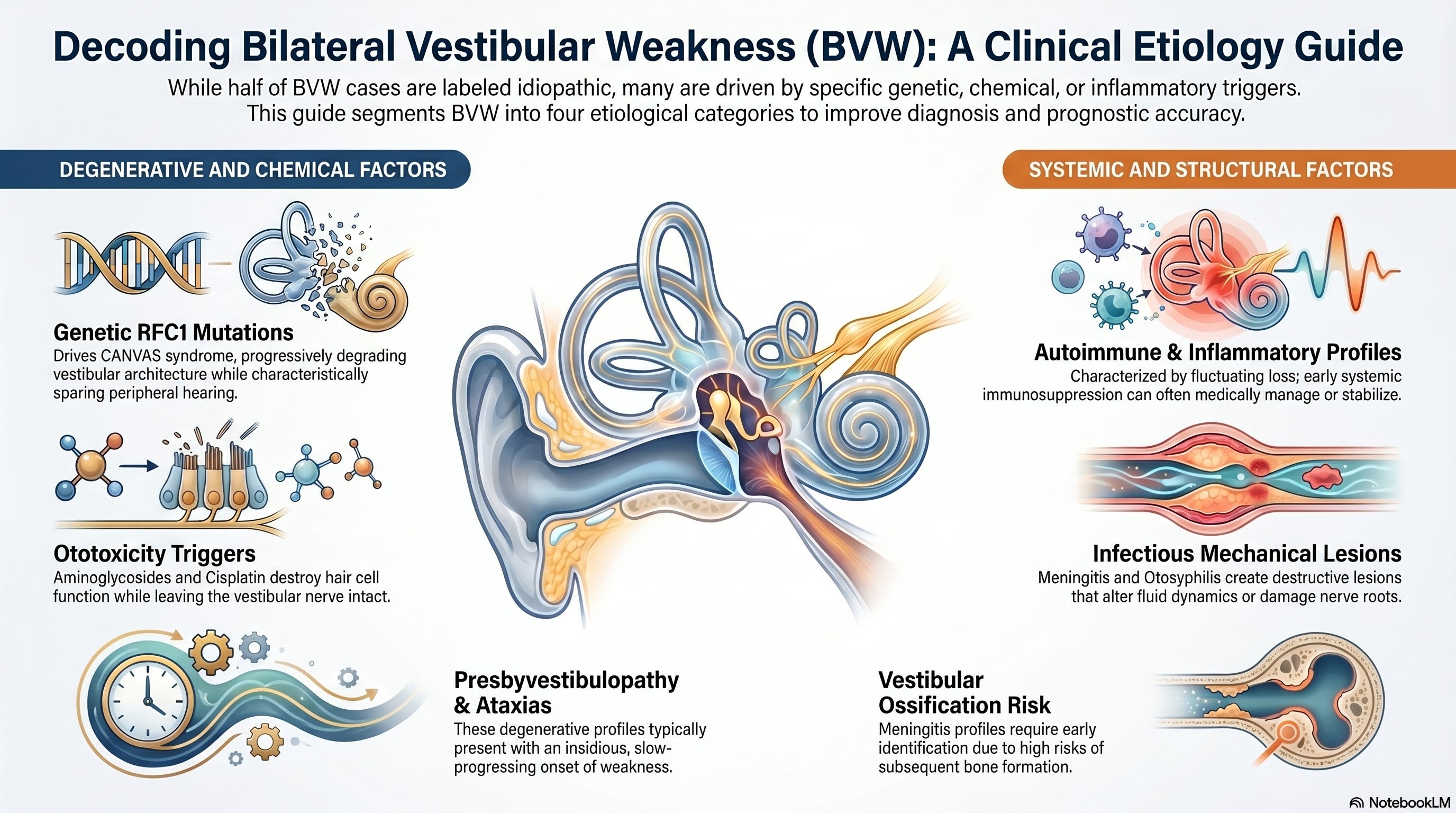
Determining the precise etiology of BVW is critical, even though up to half of all cases remain classified as idiopathic despite an exhaustive medical workup. Recent findings indicate that a substantial proportion of cases previously labeled as idiopathic are driven by RFC1 mutations, which map directly to Cerebellar Ataxia, Neuropathy, and Vestibular Areflexia Syndrome (CANVAS). To clear clinical confusion and establish realistic prognostic timelines, clinicians should separate the presentation of BVW into distinct etiological categories:
1. Genetic and Degenerative Factors:
This profile includes RFC1 mutations (CANVAS), presbyvestibulopathy, spinocerebellar ataxias, Friedreich ataxia, and Usher syndrome. These conditions typically present with an insidious onset. For instance, CANVAS characteristically spares peripheral hearing pathways while progressively degrading the central cerebellar and peripheral vestibular architecture.
2. Ototoxicity Triggers:
Key culprits include aminoglycoside antibiotics (particularly gentamicin), cisplatin, amiodarone, and chronic high-dose aspirin. The pathology involves rapid or gradual neuroepithelial destruction. This often leaves the anatomical structure of the vestibular nerve intact while completely destroying the function of the peripheral end-organ hair cells.
3. Autoimmune and Inflammatory Profiles:
This category covers autoimmune inner ear disease (AIED), chronic inflammatory demyelinating polyradiculoneuropathy (CIDP), and neurosarcoidosis. These conditions frequently present with fluctuating, rapidly progressive, or sequential asymmetric bilateral loss. Crucially, these are among the few profiles that can be medically managed or stabilized with aggressive systemic immunosuppression if caught early.
4. Infectious and Structural Alterations:
Examples include bacterial or aseptic meningitis, otosyphilis, large vestibular aqueduct syndrome, and superficial siderosis. These present with destructive mechanical or inflammatory lesions that alter endolymphatic fluid dynamics or directly damage the nerve root entry zones within the brainstem. Meningitis profiles are associated with a high risk of subsequent vestibular ossification, making early identification vital.
What Mechanisms Drive Recovery In Vestibular Rehabilitation Therapy?
Because most causes of BVW are static and irreversible, management focus must pivot away from a ‘cure’ or complete ‘restoration’ of native tissue. Instead, clinicians must use targeted strategies designed to optimize the central processing environment and support the integration of remaining sensory inputs.
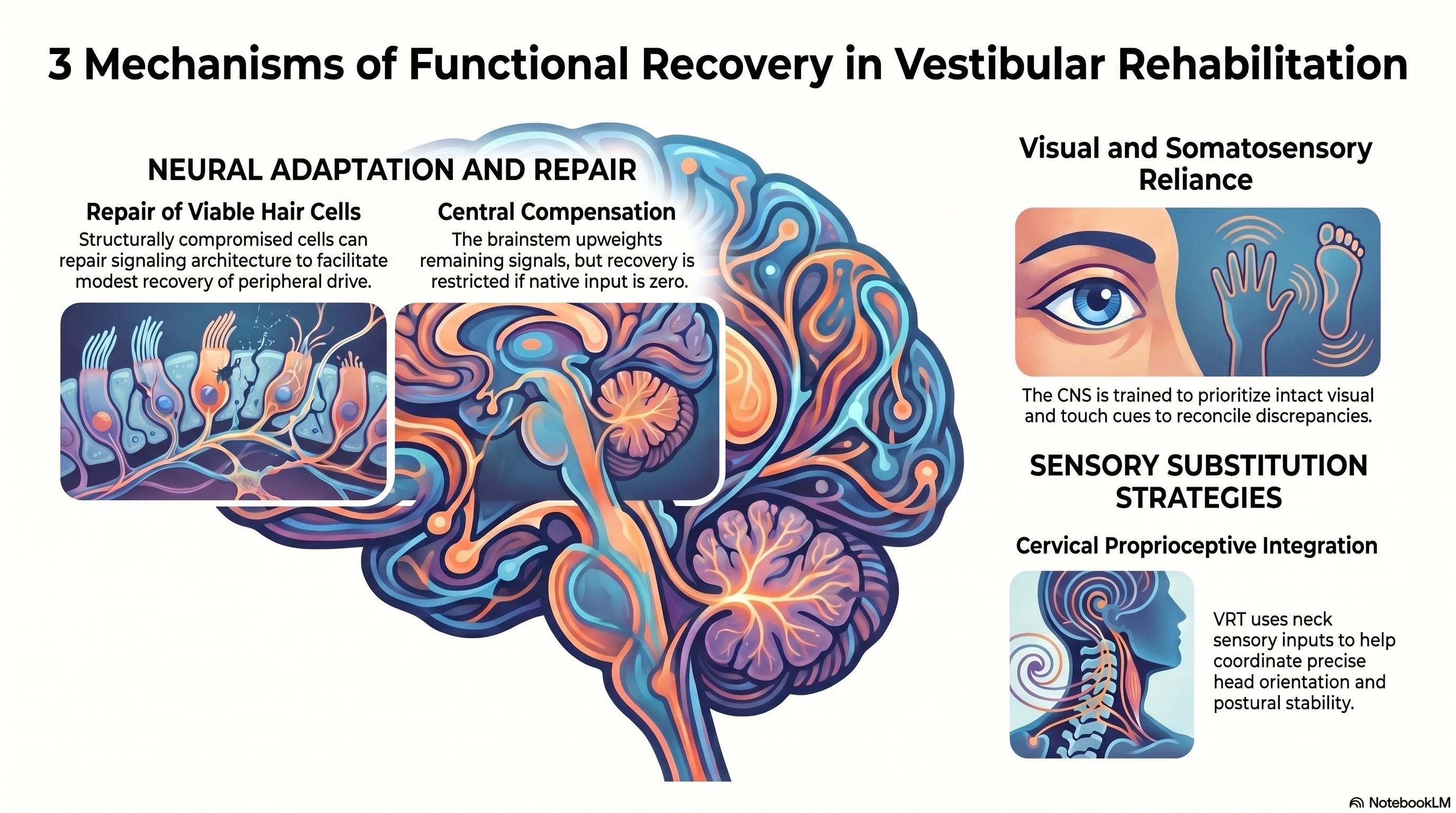
Vestibular rehabilitation therapy (VRT) leverages three primary physiological mechanisms to facilitate functional recovery:
1. Repair of Damaged Hair Cells:
While dead mammalian hair cells do not spontaneously regenerate, structurally compromised but still viable cells have a limited capacity to repair their internal signaling architecture, which can facilitate a modest recovery of peripheral drive.
2. Central Compensation:
The brainstem structures attempt to upweight the gain of any remaining peripheral vestibular signals. This mechanism is mediated by commissural pathways between the vestibular nuclei. However, control systems modeling reveals that central compensation is more severely restricted in BVW than in unilateral losses; it requires a baseline level of residual native vestibular input, as the central nervous system cannot upweight zero input.
3. Sensory Substitution:
When peripheral vestibular drive is lost, the central nervous system must rely more heavily on intact visual and somatosensory inputs to reconcile inter-sensory discrepancies. VRT formally trains this process, helping patients substitute visual cues and cervical proprioceptive inputs to coordinate precise head orientation and optimize postural stability.

Can Noisy Galvanic Vestibular Stimulation Lower Balance Thresholds?
Noisy galvanic vestibular stimulation (nGVS) represents a significant shift in neurophysiological management. While stochastic variability (random noise) typically impairs biological signal processing, the nervous system can exploit low levels of zero-mean white noise to enhance weak signals.
This phenomenon is known as ‘stochastic resonance’ or ‘stochastic facilitation’.
By delivering a weak, imperceptible electrical current via electrodes placed over the mastoid processes, nGVS lowers the vestibulospinal and perceptual thresholds required to elicit balance-related reflexes. Clinical trials demonstrate that nGVS can optimize static stance parameters, reduce postural sway, and coordinate smoother gait mechanics, particularly at slower walking speeds.
Crucially, this intervention is effective only in patients with residual vestibular function. If a complete bilateral vestibular loss exists, nGVS cannot lower reflex thresholds, as there are no remaining primary afferents to sensitize.

What Role Will Vestibular Prosthetic Implants Play In Future Protocols?
For patients with complete peripheral destruction who derive no benefit from VRT or nGVS, multi-channel vestibular prostheses offer an investigative pathway to bypass the damaged labyrinth entirely.
These implantable devices use miniature gyroscopes to sense head rotation and translate that kinetic data into patterned electrical currents. The device delivers these signals directly to the first-order neurons of the vestibular nerve branches.
Clinical trials demonstrate that vestibular implants can support a partial recovery of the rotational VOR across multiple frequencies and successfully encode high-velocity head movements. Because these devices rely entirely on the structural integrity of the eighth cranial nerve, they are highly effective for end-organ destruction (e.g., aminoglycoside ototoxicity) but will fail in conditions in which the pathology destroys the vestibular nerve itself, such as bilateral vestibular schwannomas or advanced superficial siderosis.
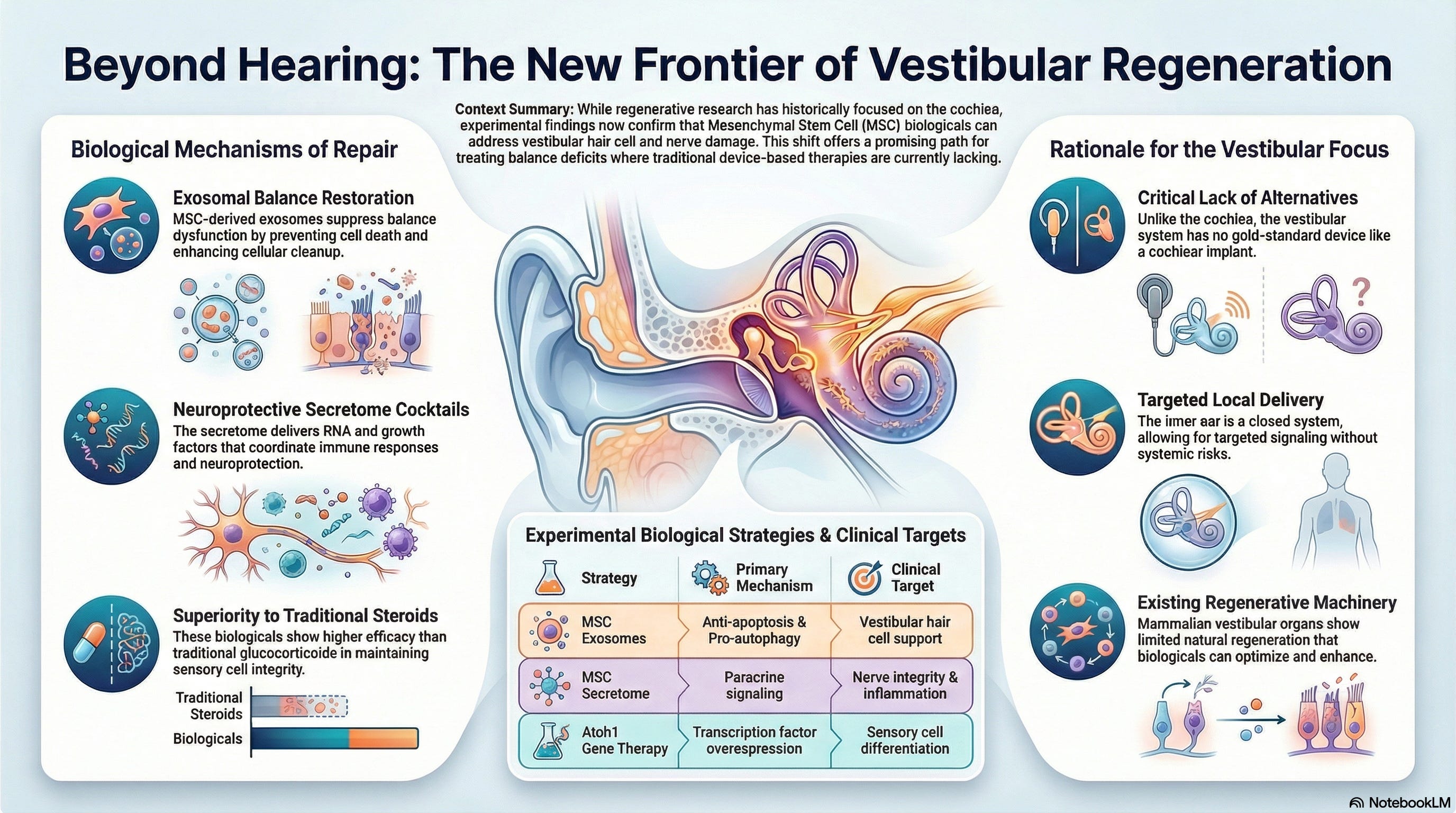
What Is The Status Of Vestibular Hair Cell Regeneration Research?
Experimental research is currently investigating molecular methods to stimulate true biological recovery. Avian models possess an innate ability to undergo mitosis of sustentacular (supporting) cells, which then transdifferentiate into functional hair cells following trauma. In mammalian models, this process is dormant.
To unlock this pathway, investigators use viral vectors to transfect the transcription factor Atonal Homolog 1 (Atoh1/Math1) into chemically ablated inner ears. In vitro and animal models demonstrate that overexpressing this gene can facilitate the growth of new vestibular hair cells and coordinate a measurable recovery of balance reflexes.
While this biological signaling approach remains strictly experimental and is not yet available in human trials, it represents the primary long-term avenue for true structural optimization of the peripheral vestibular system.
References
Cherchi, M. (2026). Bilateral vestibular weakness and its management. Current Treatment Options in Neurology, 28(5), 1-18.
Furman, J. M., & Kamerer, D. B. (1989). Rotational responses in patients with bilateral caloric reduction. Acta Oto-Laryngologica, 108(5-6), 355-361.
Karabulut, M., van Soest, A., Stultiens, J. J. A., Guinand, N., Perez Fornos, A., van de Berg, R., & et al. (2025). Vestibular implants: The present status and future prospects. In P. Kumar, N. K. Singh, M. Grover, & S. N. Dutt (Eds.), Advances in Implantation Otology (pp. 553-571). Springer Nature Singapore.
Lorente-Piera, J., Manrique-Huarte, R., de Miguel, Á. R., Ramos-Macías, Á., Robaina, S. B., Picciafuoco, S., & et al. (2026). Decoding the bilateral vestibulopathy spectrum: Etiology-based phenotypes, clinical profiles and pathways to implant candidacy. Frontiers in Neurology, 17, 1745221.
Staecker, H., Praetorius, M., Baker, K., & Brough, D. E. (2007). Vestibular hair cell regeneration and restoration of balance function induced by math1 gene transfer. Otology & Neurotology, 28(2), 223-231.
Strupp, M., Kim, J. S., Murofushi, T., Straumann, D., Jen, J. C., Rosengren, S. M., & et al. (2017). Bilateral vestibulopathy: Diagnostic criteria Consensus document of the Classification Committee of the Barany Society. Journal of Vestibular Research, 27(4), 177-189.
Tarnutzer, A. A., Bockisch, C. J., Buffone, E., & Weber, K. P. (2018). Hierarchical cluster analysis of semicircular canal and otolith deficits in bilateral vestibulopathy. Frontiers in Neurology, 9, 244.