


Unraveling the Paradox: When The Dix-Hallpike Test Goes Downbeat

In vestibular diagnostics, the Dix-Hallpike Test, developed by Margaret Dix, MD, and Charles Hallpike, MD, in 1952, reigns supreme. It's the cornerstone of assessing Benign Paroxysmal Positional Vertigo (BPPV), a common disorder causing brief episodes of dizziness triggered by head movements. We've all performed countless Dix-Hallpike tests, confidently anticipating the characteristic upbeat-torsional nystagmus that confirms our suspicions of posterior canal BPPV in the anterior arm.
But what happens when the expected pattern doesn't appear? What if, as we lower our patient to the right, we're greeted with a seemingly downbeat nystagmus, perhaps with a hint of leftward torsion? The familiar becomes unfamiliar, and we question our understanding of BPPV.

This scenario, though rare, presents a fascinating challenge for vestibular professionals. It forces us to delve deeper into the intricacies of canal mechanics, inhibitory nystagmus, and the interplay of neural pathways within the vestibular system.
Ewald's Laws: The Foundation Lies Simply in Hair Cell Orientation

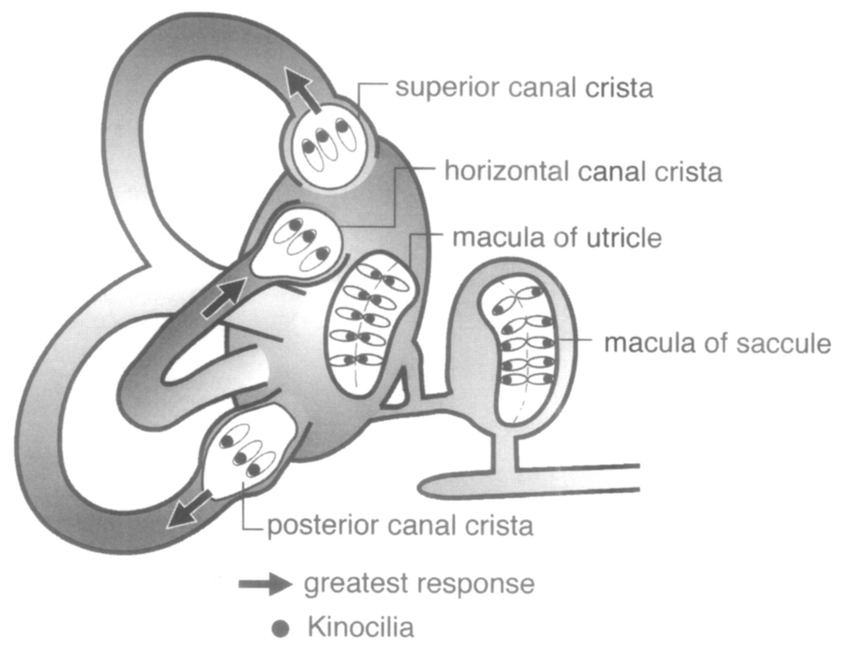
To understand this unusual presentation, we must first revisit Ewald's laws of canal function. These laws describe the relationship between endolymph flow within the semicircular canals and the resulting eye movements.
Ewald's First Law: This law states that each semicircular canal, when stimulated, will move the eyes in a plane parallel to the plane of that canal. In other words, the anatomical orientation of a canal determines the direction of the resulting nystagmus. This principle is essential for understanding how specific nystagmus patterns can help us identify which canal is affected in BPPV.
Ewald's Third Law: This law, particularly relevant to our case, states that in the vertical canals (anterior and posterior), ampullopetal flow (towards the ampulla) generates a weaker, inhibitory response. Conversely, ampullofugal flow (away from the ampulla) produces a more robust, excitatory response. This is due to the orientation of the hair cells within the crista ampullaris of the vertical canals, which is opposite to that of the horizontal canals.
Excitatory and Inhibitory Nystagmus: Asprella-Libonati's Contribution
Building on Ewald's laws, Asprella-Libonati's work further illuminated our understanding of canal function. He demonstrated that each canal can generate excitatory and inhibitory nystagmus, depending on the direction of endolymph flow.
This means that ampullopetal flow (towards the ampulla) inhibits the vertical canals, while ampullofugal flow (away from the ampulla) causes excitation.
Nystagmus and Canal Specificity
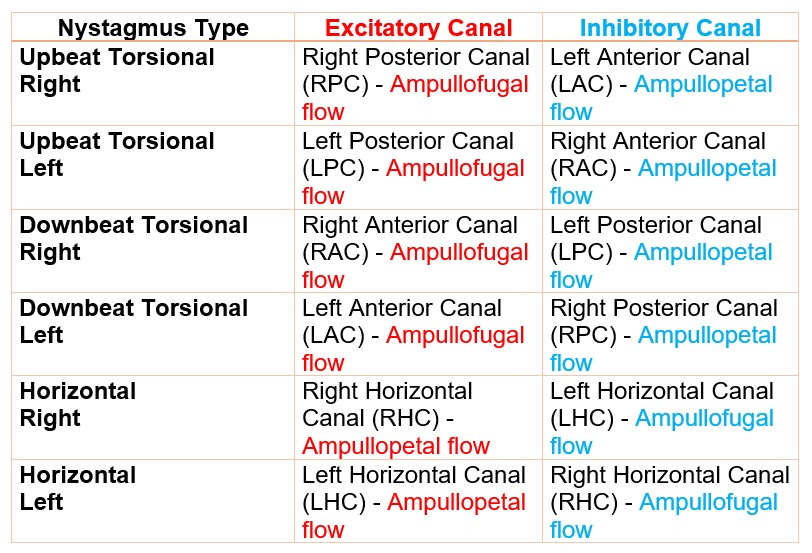
Here's where we connect the dots: Every type of nystagmus can be produced by either exciting one canal or inhibiting its paired counterpart. To illustrate this, let's examine the excitatory and inhibitory nystagmus patterns for each canal:
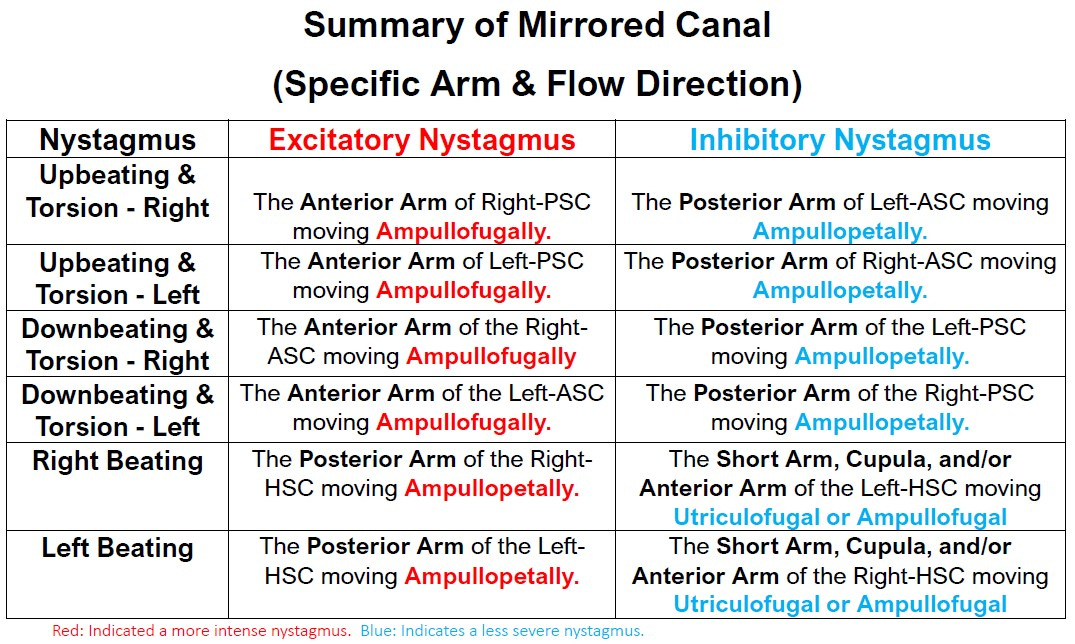
In our case of downbeat nystagmus with leftward torsion, referring to the table, we can see this could be caused by:
Debris in the Anterior Arm of the Left-ASC moving ampullofugally.
Debris in the Posterior Arm of the Right-PSC moving ampullopetally.

Ampullopetal Flow and the Vertical Canals
Why does ampullopetal flow in the vertical canals cause inhibition? The answer lies in the orientation of the hair cells within the ampulla. In the vertical canals, these hair cells are positioned such that ampullopetal flow deflects them in a way that leads to inhibition.
Connecting it to Our Case
When debris moves into the posterior arm of the posterior canal during the Dix-Hallpike maneuver to the right, it causes endolymph to flow toward the ampulla (ampullopetal flow). This inhibits the right posterior canal, resulting in the seemingly paradoxical downbeat nystagmus with leftward torsion.
The "Secret" Inhibitory Pathway: Short Arm of the Posterior Canal

Another possible explanation for this unusual nystagmus pattern involves the short arm of the posterior canal. Research by Buki et al. (2012) suggests that debris moving within the short arm can also cause ampullopetal deflection of the cupula, leading to inhibition of the posterior canal.
LARP/RALP Planes and Neural Tension
It's also important to consider the concepts of LARP (left anterior, right posterior) and RALP (right anterior, left posterior) planes, representing pairs of canals with reciprocal inhibitory relationships. Imbalances in neural activity between these paired canals can influence nystagmus.
Central Causes and Differential Diagnosis
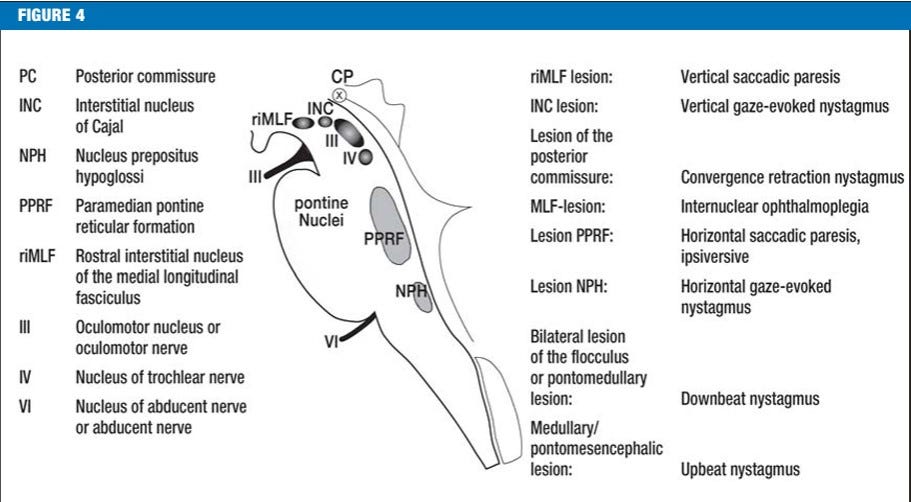
While our focus has been on peripheral vestibular causes, it's crucial to remember that downbeat nystagmus can also be a sign of central pathology. The differential diagnosis should consider conditions such as cerebellar or pontomedullary lesions.
Conclusion
This atypical Dix-Hallpike finding highlights the complexities of vertical canal BPPV and underscores the importance of understanding inhibitory nystagmus. By integrating knowledge of Ewald's laws, Asprella-Libonati's work, and the intricacies of ampullopetal flow, we can decipher these unusual presentations and provide more accurate diagnoses and targeted interventions.