


Unveiling the Casani and BASTORE Maneuvers: Liberating Solutions for Short-Arm Cupulolithiasis

Introduction:
Benign Paroxysmal Positional Vertigo (BPPV) is a common vestibular disorder that can significantly impact a person's quality of life. While traditional maneuvers like the Epley and Semont have proven effective for many BPPV cases, they might not be successful when the culprit is debris attached to the short arm of the cupula or potentially lodged in the ampullary segment. This article introduces two novel and specialized maneuvers designed to address these unique scenarios: the Casani maneuver for horizontal canal BPPV and the BASTORE maneuver for posterior canal BPPV.
The Challenge of Short-Arm Cupulolithiasis
In most BPPV cases, dislodged otoconia (calcium carbonate crystals) adhere to the long arm of the cupula, a sensory structure within the semicircular canals. However, in some instances, this debris can attach to the short arm or become trapped within the ampullary segment, closer to the utricle. Traditional maneuvers might struggle to effectively dislodge debris from these locations, leading to persistent vertigo and treatment failures.
Casani Maneuver: A Quick, Forceful Push
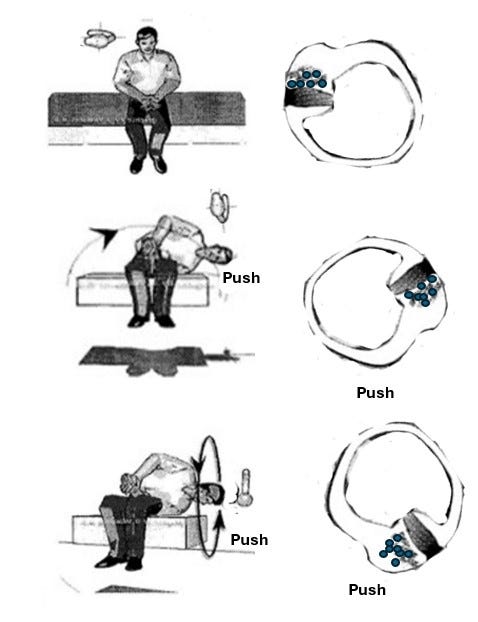
The Casani maneuver addresses horizontal canal BPPV with short-arm cupulolithiasis or potential ampullary debris. It involves a rapid, dynamic movement to shake the debris loose and guide it back into the utricle.
The Maneuver:
The patient starts in a seated position with their head straight.
They quickly lie down on their unaffected side, keeping their head straight.
Immediately after lying down, the head is briskly turned downwards (Gufoni position).
The patient remains in this position 1-2 minutes, allowing gravity to move debris into the utricle.
They then slowly return to an upright position.
Mechanism: The rapid head movement creates a sudden shift in fluid dynamics within the horizontal canal, dislodging the debris from the short arm or ampulla.
BASTORE Maneuver: A Gentle, Repetitive Approach
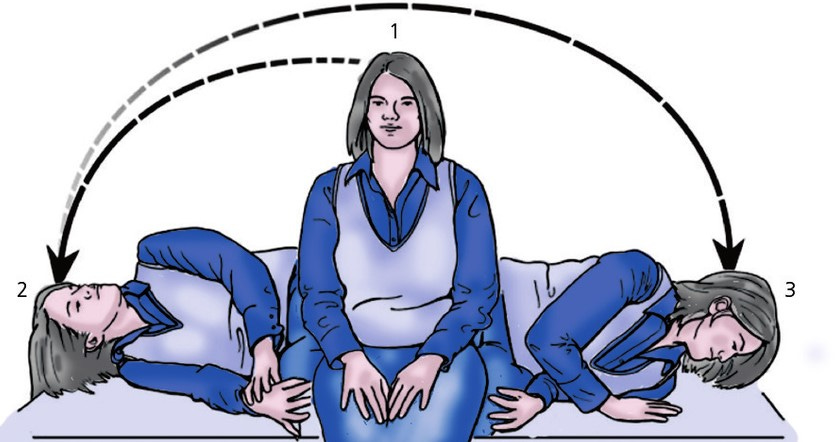
The BASTORE maneuver (Bi-directional Arm Semont Therapy with Opposite Repositioning Exercise) targets posterior canal BPPV with short-arm cupulolithiasis or potential ampullary involvement. It utilizes a more gradual, repetitive approach, mimicking a reversed Semont maneuver.
The Maneuver:
The patient sits with their head turned 45 degrees from the affected ear.
They are quickly laid down on the affected side, maintaining the head turn.
The head is then rotated downwards towards the floor.
The patient rolls onto the opposite side, keeping the head in the same downward position.
They slowly sit up, maintaining the head turn.
This sequence is repeated several times.
Mechanism: The repeated head movements create a push-pull effect on the cupula, gradually dislodging the debris and guiding it back into the utricle.
Key Points to Remember:
Accurate Diagnosis: Both maneuvers require a precise diagnosis by a qualified healthcare professional to ensure appropriate application.
Professional Guidance: To ensure safety and effectiveness, these maneuvers should be performed under the supervision of a trained clinician.
Patient Education: Explaining the maneuvers and their potential sensations to the patient can alleviate anxiety and enhance cooperation.
Follow-up: Regular follow-up appointments are essential to monitor progress and adjust treatment if necessary.
Conclusion:
The Casani and BASTORE maneuvers offer promising treatment options for BPPV cases involving short-arm cupulolithiasis or potential ampullary debris. By understanding the unique challenges posed by these scenarios and employing these specialized techniques, healthcare professionals can provide targeted relief and improve the quality of life for individuals with BPPV.