
📝 Unwinding the Maladaptive Loop: How Vestibular Dysfunction Drives Cervical Dystonia


The human body possesses a magnificent, complex capacity for adaptation. When injury strikes, the Central Nervous System (CNS) consistently prioritizes stability, survival, and perception. However, the strategies it develops to achieve stability can, over time, become pathological. This concept is vividly illustrated in the case of a patient presenting with chronic, agonizing cervical dystonia rooted in a vestibular hypofunction, coexisting with severe degenerative joint disease (DJD).
The Confluence of Chaos: Vestibular Failure and Cervical Instability
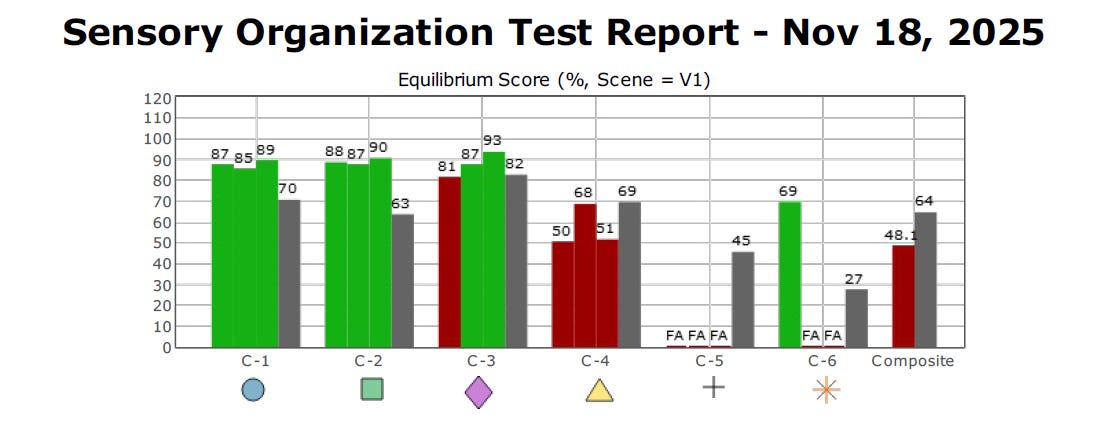
A patient presented with severe cervical pain and dystonia following a documented right-sided vestibular hypofunction. Diagnostic evidence from Computerized Dynamic Posturography (CDP) confirmed a profound balance deficit, characterized by a Visual-Vestibular Mismatch (VVM) sensory strategy, as classified by the FYZICAL Balance Paradigm. The Composite Score of 48.1% places her squarely in this VVM category, indicating an over-reliance on the visual system to compensate for a failing vestibular system.
Furthermore, the patient demonstrated classic signs of otolithic dysfunction—a link confirmed by her complaint of postural hypotension. The crucial connection here is the Vestibulo-Sympathetic Reflex (VSR), which uses otolithic input to regulate blood pressure. A compromised otolithic system fails to activate the VSR properly, leading to orthostatic intolerance.
The chronic cervical dystonia, however, constitutes the most debilitating symptom. The initial right-sided vestibular injury created a tonic asymmetry, which drove a pathological left-beating nystagmus.
The brain perceived a continuous rotation. In an attempt to correct this perceived spin and achieve stability, the CNS, contending with painful, noisy, and corrupted somatosensory input from the cervical DJD, developed a sustained, involuntary muscle contraction. This is the definition of dystonia—a maladaptive motor strategy that creates its own source of ‘agonizing pain and instability‘.
Breaking the Cycle with Optokinetic Flow and Controlled Dosage
Traditional Vestibular Rehabilitation Therapy (VRT) often focuses on habituation and gaze stabilization. However, treating this complex case requires a more direct, powerful intervention to unwind the maladaptive motor strategy. The solution involves introducing a controlled, therapeutic sensory error signal using optokinetic flow.
The patient’s pathology is driven by a tonic imbalance causing a left-beating nystagmus and a physical pull to the left. To counter this, the therapist must induce a powerful, yet false, sensation of turning to the right. The therapist uses an optokinetic bar system to project a visual flow moving from Right to Left (R to L), which generates a powerful illusion of self-motion—called vection—causing the patient to feel like they are turning to the right. The brain integrates this massive rightward vection signal with the pathological leftward signal, effectively driving a compensatory motor output to relax the left-sided dystonic tension.
The application of this technique requires a careful, dose-dependent progression, with cervical pain acting as the tolerance benchmark:
Initial Dosage: The patient performs the exercise for 1 minute at a time, completing 3 sets (3 minutes total) once per day.
Progression: The therapist increases the dosage only if the patient reports no increase in cervical pain or stiffness for 3 consecutive days. If this condition is met, the therapist adds one 3-minute set, progressing the patient to twice per day.
Maximum Target Dosage: If the patient remains asymptomatic for three additional days, the therapist adds a final set, resulting in the patient performing the exercise three times per day for 3 minutes per session, totaling 9 minutes daily.
By introducing this controlled, dose-dependent visual challenge, the therapist is providing the brain with the precise, high-gain signal it needs to recognize and abandon its maladaptive dystonic strategy. The aim is to achieve the CNS adaptation necessary for the brain to recalibrate, restoring automatic, unconscious postural control and finally breaking the ‘agonizing cycle of pain and instability‘.
As one of my mentors often stated, ‘The central nervous system must be challenged in a precise, dose-dependent manner to achieve true, lasting neuroplastic change.‘
Brian K. Werner, PT, MPT, Bio:
Brian Werner, PT, MPT, is a physical therapist who has been specializing in vestibular and balance disorders for over a quarter of a century. He is the founder of the FYZICAL Balance Paradigm and one of the co-founders of FYZICAL, LLC, Balance Center Division with Dr. Daniel Deems, MD, PhD, where he serves as the National Director of Vestibular Education & Training.
Question: When the patient look at the bars where do they start? At the first bar and go all the way to the end? Or do they start in the middle and continue to the end? I know that the movements of the eyes would be more challenged the closer they start at the end of the bars. What would you recommend?