

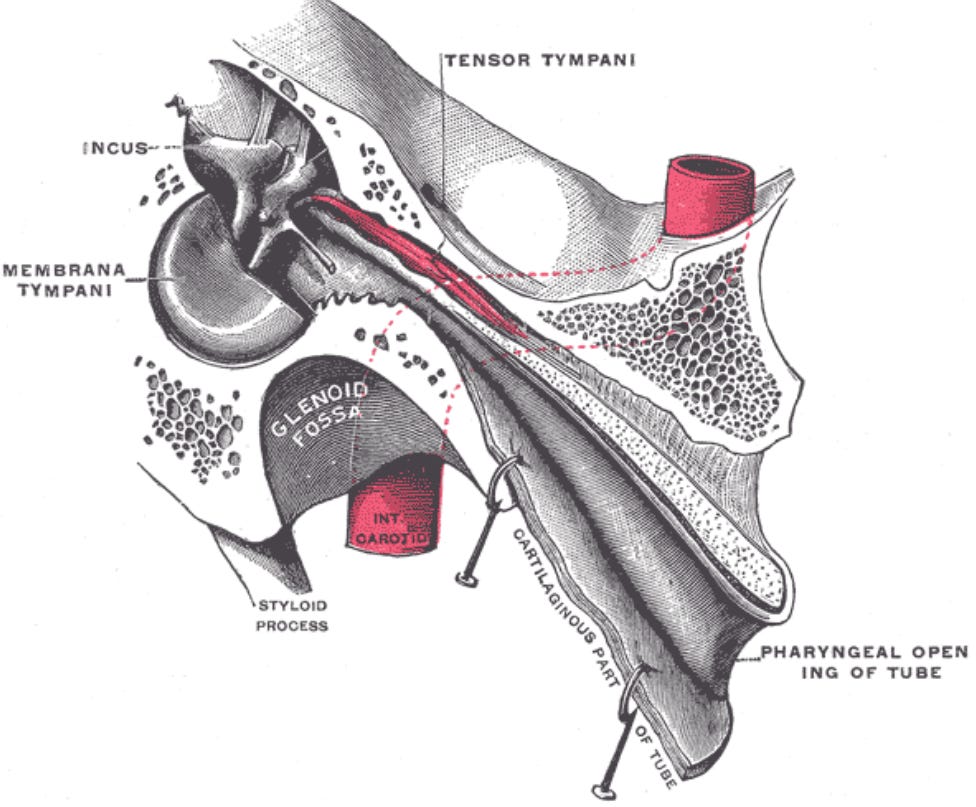
The tensor tympani is a striated muscle innervated by the motor division of the trigeminal nerve. Under normal physiological conditions, the muscle contracts reflexively during swallowing, chewing, and vocalization to reduce the transmission of low-frequency sound. However, when the centrally mediated reflex threshold is lowered, the muscle enters tonic hypertonicity (Westcott et al., 2013). This chronic contraction pulls the manubrium of the malleus medially, stretching the tympanic membrane inward.
This structural displacement alters the mechanical impedance of the ossicular chain and directly loads the somatosensory mechanoreceptors embedded within the eardrum mucosa (Londero et al., 2017).
The brain receives continuous afferent feedback through the trigeminal pathway, which it misinterprets as an environmental pressure gradient or physical blockage. Because this phenomenon is entirely myogenic rather than hydrostatic, patients report that the Valsalva maneuver fails to provide even temporary clearance.

What Clinical Research Confirms Myogenic Aural Fullness?
Epidemiological and physiological evidence heavily supports the role of middle ear muscle hypertonicity in generating false pressure signals. In a comprehensive multi-clinic study, researchers analyzed the symptom profiles of patients exhibiting signs of chronic tensor tympani hypertonicity (Westcott et al., 2013).
The investigation revealed that aural fullness and a sensation of ear blockage were among the most prominent secondary otological symptoms, occurring in 60.0% of the total sample and rising significantly to 81.1% in patients with decreased sound tolerance.
Furthermore, physiological modeling demonstrates that non-auditory trigeminal stimulation increases ossicular stiffness and shifts the tympanic membrane position, driving changes in mechanical impedance that mirror the effects of ambient pressure changes (Londero et al., 2017). This persistent muscle tension induces localized tissue strain, which activates nociceptive and somatosensory feedback loops within the trigeminal cervical complex. This neurogenic loop amplifies the perceived physical restriction inside the ear canal, masking a pure sensorimotor response as an apparent ventilation deficit.

How Should Clinicians Address Sensorimotor Ear Pressure?
Managing this myogenic fullness requires moving away from traditional middle ear interventions such as decongestants or tympanostomy tubes, which provide no clinical benefit in the absence of fluid or negative pressure. Instead, management must focus on down-regulating the hyper-reflexive trigeminal network and reducing autonomic hypervigilance.
Clinicians should apply targeted habituation protocols and sound therapy framework tools to desensitize the lowered acoustic and somatic reflex thresholds. Addressing maladaptive sensory strategies and integrating central relaxation techniques can help stabilize the trigeminal cervical complex, ultimately releasing the tonic contraction of the tensor tympani muscle.
References
Londero, A., Charpentier, N., Ponsot, D., Fournier, P., Pezard, L., & Noreña, A. J. (2017). A case of acoustic shock with post-traumatic trigeminal-autonomic activation. Frontiers in Neurology, 8, 420. https://doi.org/10.3389/fneur.2017.00420 Cited by: 26
Westcott, M., Sanchez, T. G., Sharples, T., Diges, I., Saba, C., Dineen, R., McNeill, C., Chiam, A., & O′Keefe, M. (2013). Tonic tensor tympani syndrome in tinnitus and hyperacusis patients: A multi-clinic prevalence study. Noise and Health, 15(63), 117–128. https://doi.org/10.4103/1463-1741.110295 Cited by: 92
Have you tried bromelain with your patients ? I don't understand much of the science in this article, but would love to know more about how to support the muscle health in the ears ? I have had years of a sensation of fullness in my ears, which has been really annoying. And extreme pain on landing in a plane on occasions - but not always. (All accompanied by vestibular migraine.) I started using bromelain a few months ago, and within days, the sensation of fullness had eased. It's still there sometimes, but nowhere near as annoying as it used to be, and sometimes I can go through a whole day without thinking about my ears, which never used to happen. I'd love to know your thoughts, and also to suggest a research trial into it. A nutritionist friend recommended it to me - it's also supposed to be good for sinusitis. Also, is there a connection between ear fullness and VM ? Thanks Kate
Fascinating hypothesis. As an otologist, I certainly see patients with persistent aural fullness despite a patent Eustachian tube. The somatosensory-trigeminal contribution is biologically plausible, but I think we’re still missing high-quality mechanistic and interventional studies before this can be considered an established disease mechanism rather than one potential explanation in a subset of patients.