
⚖️ The Horizontal Canal Compass: Mastering the ‘Geo Most, Apo Least’ Rule (Edited 12/27)


Assessing Horizontal Canal Benign Paroxysmal Positional Vertigo (HC-BPPV) demands a precise yet straightforward diagnostic tool. While the neurophysiological mechanics can be complex, vestibular professionals use a fundamental clinical rule, the ‘Geo Most, Apo Least’ concept, to instantly determine the affected ear during the Supine Head Roll Test (Pagnini-McClure Test).
This rule focuses solely on the ‘intensity’ of the nystagmus and its ‘direction’ (Geotropic or Apogeotropic) to guide your treatment.
The Historical Context of BPPV Nystagmus
We recognize that all positional nystagmus associated with BPPV—whether arising from the horizontal, posterior, or anterior canals—contains a geotropic (towards the earth) or apogeotropic (away from the planet) vector. This distinction arises from the relationship between the debris movement and the plane of the specific canal in the testing position.
For instance, Posterior Canal BPPV (diagnosed via Dix-Hallpike), which produces upbeat, torsional nystagmus, carries a geotropic component. Anterior Canal BPPV, which produces downbeat, torsional nystagmus, carries an apogeotropic component.
However, the specific, purely horizontal descriptive terms ‘Geotropic’ (beating towards the ground) and ‘Apogeotropic’ (beating away from the ground) are most famously and clearly defined when assessing the Horizontal Canal during the Supine Head Roll Test. The geotropic variant of HC-BPPV was first described by McClure (1985), and the apogeotropic variant was later described by Baloh et al. (1995). Theoretical explanations for these atypical pathologies are well-detailed in the literature (Büki et al., 2014). They form the basis of the ‘Geo Most, Apo Least’ clinical rule.
The Supine Head Roll Test and Nystagmus Direction
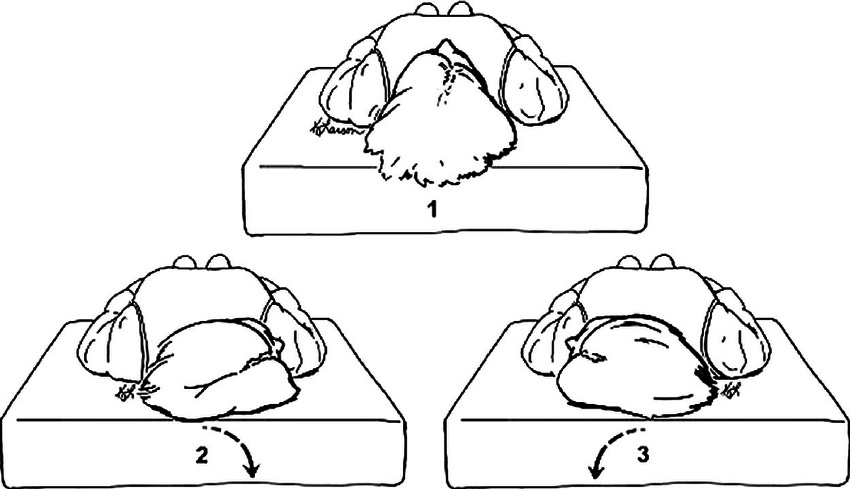
During the Supine Head Roll Test, we turn the patient’s head to the right, then to the left, and observe the induced nystagmus while maintaining approximately 30 degrees of cervical flexion to keep the canals perpendicular to the ground, optimizing the test.2 The direction of the nystagmus relative to the ground defines the type of HC-BPPV:
Geotropic Nystagmus (Geo): The nystagmus beats toward the earth (down toward the pillow) in both head-turn positions. This pattern indicates Canalithiasis, where debris is loose within the long arm (specifically the posterior segment) of the canal.
Apogeotropic Nystagmus (Apo): The nystagmus beats away from the earth (up toward the ceiling) in both head-turn positions.3 This pattern indicates Cupulolithiasis (debris adhering to the cupula) or Canalithiasis located in the short arm, periampullary region, or in the anterior segment/ampullary segment of the horizontal canal.
Applying the Simple Rule: ‘Geo Most, Apo Least’
The core strength of this rule is its focus on the dependent ear—the ear closest to the ground—which you test with the head turn. If you turn the head right, you test the right ear; if you turn the head left, you test the left ear. This prevents the common diagnostic confusion that arises when trying to relate nystagmus to the upward (non-dependent) ear.
The rule allows you to identify the affected side by simply comparing the intensity and duration of the nystagmus in the right-head-turn and left-head-turn positions.
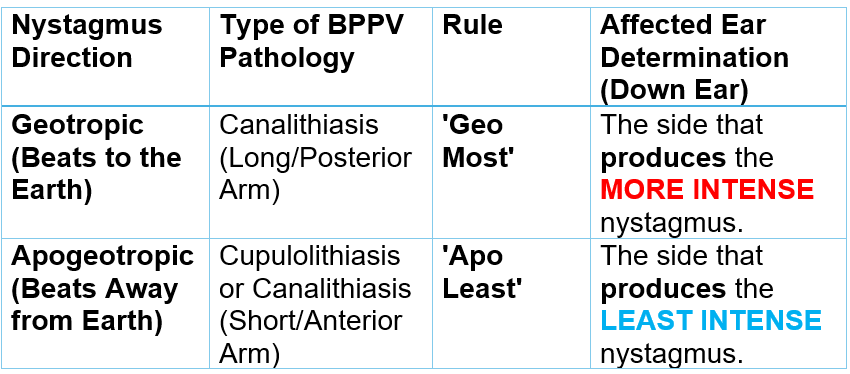
1. Geotropic Nystagmus: ‘Geo Most.’
Geo Most states that when the nystagmus is Geotropic, the side that produces the MORE INTENSE nystagmus is the affected ear.
The Rationale: When the affected ear is down, gravity causes debris to flow ampullopetally (toward the ampulla), thereby generating a strong excitatory stimulus. This generates the more intense nystagmus in the tested (downward) ear.
2. Apogeotropic Nystagmus: ‘Apo Least.’
Apo Least states that when the nystagmus is Apogeotropic, the side that produces the LEAST INTENSE nystagmus is the affected ear.4
The Rationale: When the affected ear is down, gravity causes the debris to flow ampullofugally (away from the ampulla) or deflect the cupula in an inhibitory direction. This creates an inhibitory stimulus, leading to less intense nystagmus in the tested (downward) ear.
Clinical Summary Table
This table summarizes how you use the ‘Geo Most, Apo Least’ rule to identify the affected ear.
Important Note
We recognize there are many ways to analyze and interpret nystagmus. This ‘Geo Most, Apo Least’ method provides a direct and efficient clinical shortcut when performing the Supine Head Roll Test. Other methods, such as the Excitatory Nystagmus Concept, offer a deeper neurophysiological perspective, which we will explore in a future article.
Conclusion: Purpose Tip for Professionals
The difference between a successful repositioning maneuver and a frustrating failure often rests on correctly identifying the affected side. Mastering the ‘Geo Most, Apo Least’ framework empowers vestibular professionals to triage HC-BPPV rapidly, select the appropriate maneuver (such as the Gufoni or the full roll), and deliver immediate, effective relief to the patient. Use this simple comparison of nystagmus intensity to ensure a precise diagnosis every time.
References
Baloh, R. W., Honrubia, V., & Jacobson, K. (1995). Benign positional vertigo: clinical and oculographic features in 240 cases. Neurology, 45(10), 1801–1807.
Büki, B., Mandalà, M., & Nuti, D. (2014). Typical and atypical benign paroxysmal positional vertigo: literature review and new theoretical considerations. Journal of Vestibular Research, 24(5-6), 415–423.
McClure, J. A. (1985). Horizontal canal BPV. The Journal of Otolaryngology, 14(1 Suppl), 30–33.
Vats, Ajay & Vajpeyee, Atulabh & Ramchandani, Gd & Sharma, Jugal. (2021). Benign Paroxysmal Positional Vertigo: Diagnosis and Management by Physical Therapy and Repositioning Maneuvers.
Brian Werner, PT, MPT, is a physical therapist who has been specializing in vestibular and balance disorders for over a quarter of a century. He is the founder of the FYZICAL Balance Paradigm and one of the co-founders of FYZICAL, LLC, Balance Center Division with Dr. Daniel Deems, MD, PhD, where he serves as the National Director of Vestibular Education & Training.
I understand that this question isn’t the point of this article - but in the graphic of the supine head roll test - there is no 30 degrees of cervical flexion - how important is this to the accuracy/reliability for the test?